

Effects of transsectoral long-term neurorehabilitation
- PMID: 38326907
- PMCID: PMC10851455
- DOI: 10.1186/s42466-023-00302-3
Effects of transsectoral long-term neurorehabilitation
Abstract
Background: Acquired brain injuries are among the most common causes of disability in adulthood. An intensive rehabilitation phase is crucial for recovery. However, there is a lack of concepts to further expand the therapeutic success after the standard rehabilitation period. Hereafter, the characteristics of a transsectoral, multiprofessional long-term neurorehabilitation concept and its effects on outcome at different ICF levels are described.
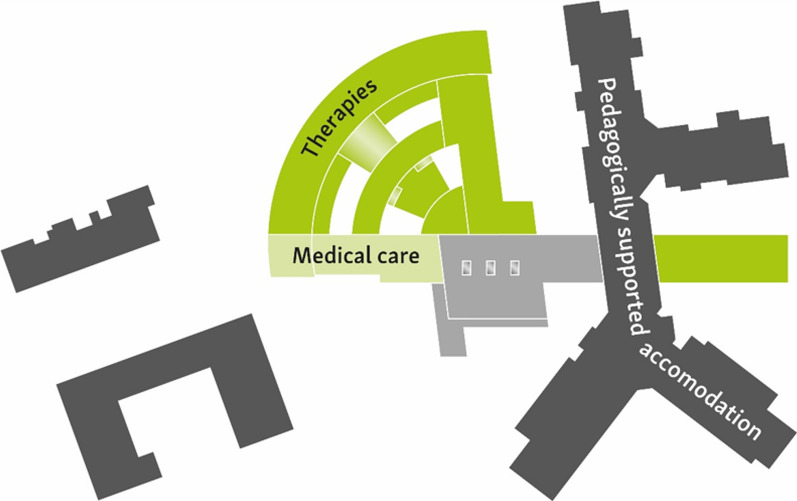
Methods: The P.A.N. Center for Post-Acute Neurorehabilitation combines living with 24/7 support of pedagogical staff with on-site outpatient therapy and medical care. A secondary data analysis was conducted on the records of all patients with completeted P.A.N. treatment between 01.01.2015 and 09.04.2022. Outcome parameters included demographic characteristics, diagnostics, Barthel Index (BI), the German scale "Hilfebedarf von Menschen mit Behinderung für den Lebensbereich Wohnen " (HMBW), the Canadian Occupational Performance Measure (COPM) and the destination after discharge. For BI and discharge destination, potential determinants of therapy success are evaluated.
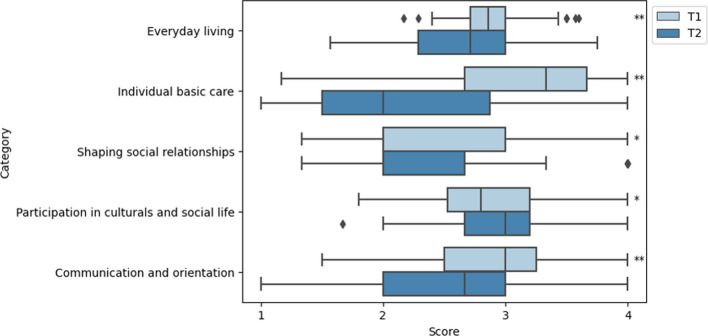
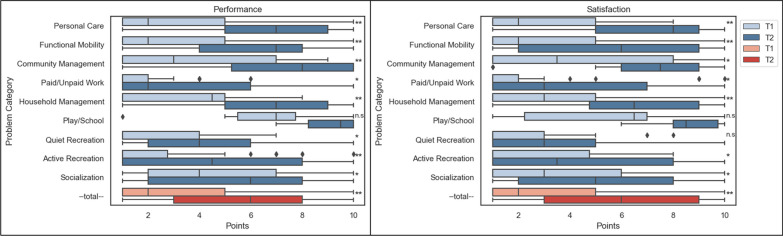
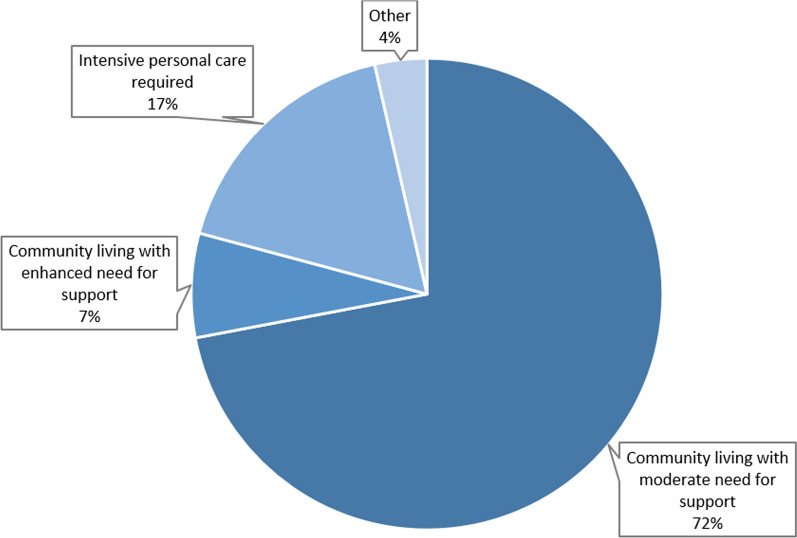
Results: 168 patients were enrolled in the analyses. Significant improvements were observed in the BI (p < .001), with median values increasing from 55 to 80 points. The HMBW showed a significant decrease in the need for assistance in everyday living (p < .001), individual basic care (p < .001), shaping social relationship (p = .003) and communication (p < .001). Significant improvements were reported in the COPM total score for performance (p < .001) and satisfaction (p < .001). 72% of the patients were able to move in a community living arrangement with moderate need for support. Main predictive factor for discharge destination was the initial cognitive deficit. The comparison of the third-person scales BI and HMBW with the self-reported COPM showed that individually formulated patient goals are only insufficiently reflected in these global scales.
Discussion: The data show that a highly coordinated, trans-sectoral 24/7 approach of goal-oriented practice as pursued at P.A.N. is feasible and effective. We assume that the success of the intervention is due to the high intensity of therapies delivered over a long time and its interlink with real world practice. For a comprehensive analysis of rehabilitation success, it is necessary to record and evaluate individual patient goals, as these are not always reflected in the commonly used global scales.
Keywords: Acquired brain injury; Chronic phase; Long-term rehabilitation; Neurorehabilitation; Stroke; Transsectoral.
© 2024. The Author(s).
Conflict of interest statement
CD and SB (until March 2022) are/were employees of the P.A.N. centre. MS, AS and TS are employees of the Fürst Donnersmarck-Stiftung, the head organisation of the P.A.N. centre. The authors declare that they have no competing interests.
Figures

References
-
- James SL, Theadom A, Ellenbogen RG, Bannick MS, Montjoy-Venning W, Lucchesi LR, et al. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet Neurology. 2019;18:56–87. doi: 10.1016/S1474-4422(18)30415-0. - DOI - PMC - PubMed
-
- Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet Neurology. 2021;20:795–820. doi: 10.1016/S1474-4422(21)00252-0. - DOI - PMC - PubMed
-
- Bundesarbeitsgemeinschaft für Rehabilitation, editor. Empfehlungen zur Neurologischen Rehabilitation von Patienten mit schweren und schwersten Hirnschädigungen der Phasen B und C. Frankfurt/Main: Bundesarbeitsgemeinschaft für Rehabilitation (1999).
LinkOut - more resources
Full Text Sources