Atherosclerotic Calcifications Have a Local Effect on the Peel Behavior of Human Aortic Media
- PMID: 38329432
- PMCID: PMC10983699
- DOI: 10.1115/1.4064682
Atherosclerotic Calcifications Have a Local Effect on the Peel Behavior of Human Aortic Media
Abstract
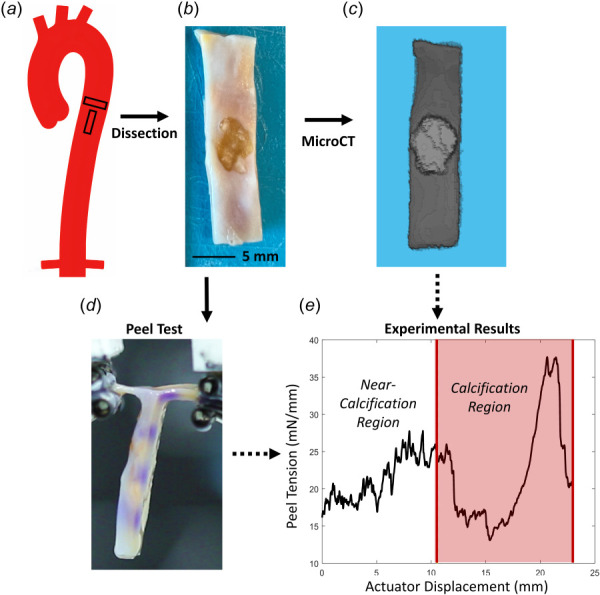
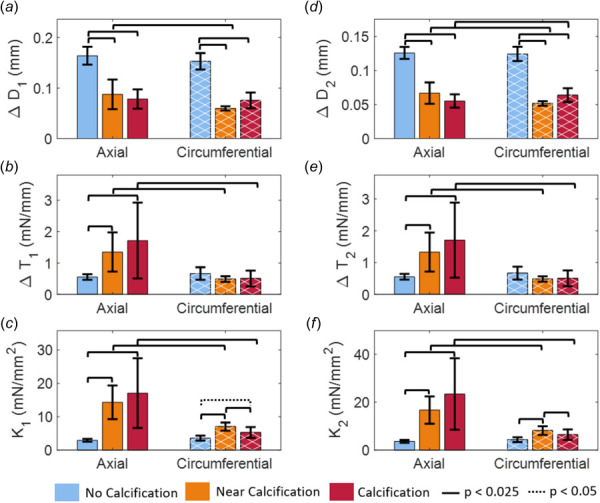
Aortic dissections, characterized by the propagation of a tear through the layers of the vessel wall, are critical, life-threatening events. Aortic calcifications are a common comorbidity in both acute and chronic dissections, yet their impact on dissection mechanics remains unclear. Using micro-computed tomography (CT) imaging, peel testing, and finite element modeling, this study examines the interplay between atherosclerotic calcifications and dissection mechanics. Samples cut from cadaveric human thoracic aortas were micro-CT imaged and subsequently peel-tested to map peel tension curves to the location of aortic calcifications. Empirical mode decomposition separated peel tension curves into high and low-frequency components, with high-frequency effects corresponding to interlamellar bonding mechanics and low-frequency effects to peel tension fluctuations. Finally, we used an idealized finite element model to examine how stiff calcifications affect aortic failure mechanics. Results showed that atherosclerosis influences dissection behavior on multiple length scales. Experimentally, atherosclerotic samples exhibited higher peel tensions and greater variance in the axial direction. The variation was driven by increased amplitudes of low-frequency tension fluctuations in diseased samples, indicating that more catastrophic propagations occur near calcifications. The simulations corroborated this finding, suggesting that the low-frequency changes resulted from the presence of a stiff calcification in the vessel wall. There were also modifications to the high-frequency peel mechanics, a response likely attributable to alterations in the microstructure and interlamellar bonding within the media. Considered collectively, these findings demonstrate that dissection mechanics are modified in aortic media nearby and adjacent to aortic calcifications.
Copyright © 2024 by ASME.
Figures







References
-
- Melvinsdottir, I. H. , Lund, S. H. , Agnarsson, B. A. , Sigvaldason, K. , Gudbjartsson, T. , and Geirsson, A. , 2016, “ The Incidence and Mortality of Acute Thoracic Aortic Dissection: Results From a Whole Nation Study,” Eur. J. Cardio-Thoracic Surg., 50(6), pp. 1111–1117.10.1093/ejcts/ezw235 - DOI - PubMed
-
- Obel, L. M. , Lindholt, J. S. , Lasota, A. N. , Jensen, H. K. , Benhassen, L. L. , Mørkved, A. L. , Srinanthalogen, R. , Christiansen, M. , Bundgaard, H. , and Liisberg, M. , 2022, “ Clinical Characteristics, Incidences, and Mortality Rates for Type a and B Aortic Dissections: A Nationwide Danish Population-Based Cohort Study From 1996 to 2016,” Circulation, 146(25), pp. 1903–1917.10.1161/CIRCULATIONAHA.122.061065 - DOI - PubMed
-
- Kälsch, H. , Lehmann, N. , Möhlenkamp, S. , Hammer, C. , Mahabadi, A. A. , Moebus, S. , and Schmermund, A., et al., 2013, “ Prevalence of Thoracic Aortic Calcification and Its Relationship to Cardiovascular Risk Factors and Coronary Calcification in an Unselected Population-Based Cohort: The Heinz Nixdorf Recall Study,” Int. J. Cardiovasc. Imaging, 29(1), pp. 207–216.10.1007/s10554-012-0051-3 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical