

Methylprednisolone as Adjunct to Endovascular Thrombectomy for Large-Vessel Occlusion Stroke: The MARVEL Randomized Clinical Trial
- PMID: 38329440
- PMCID: PMC10853866
- DOI: 10.1001/jama.2024.0626
Methylprednisolone as Adjunct to Endovascular Thrombectomy for Large-Vessel Occlusion Stroke: The MARVEL Randomized Clinical Trial
Abstract
Importance: It is uncertain whether intravenous methylprednisolone improves outcomes for patients with acute ischemic stroke due to large-vessel occlusion (LVO) undergoing endovascular thrombectomy.
Objective: To assess the efficacy and adverse events of adjunctive intravenous low-dose methylprednisolone to endovascular thrombectomy for acute ischemic stroke secondary to LVO.
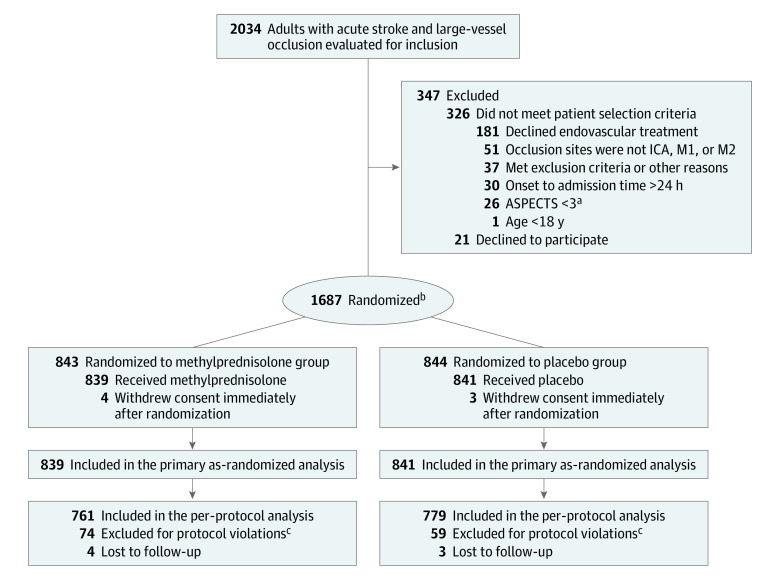
Design, setting, and participants: This investigator-initiated, randomized, double-blind, placebo-controlled trial was implemented at 82 hospitals in China, enrolling 1680 patients with stroke and proximal intracranial LVO presenting within 24 hours of time last known to be well. Recruitment took place between February 9, 2022, and June 30, 2023, with a final follow-up on September 30, 2023.
Interventions: Eligible patients were randomly assigned to intravenous methylprednisolone (n = 839) at 2 mg/kg/d or placebo (n = 841) for 3 days adjunctive to endovascular thrombectomy.
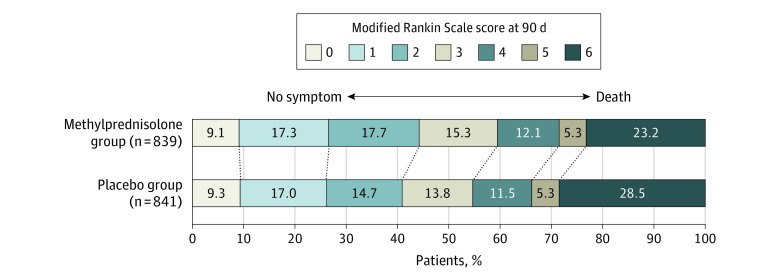
Main outcomes and measures: The primary efficacy outcome was disability level at 90 days as measured by the overall distribution of the modified Rankin Scale scores (range, 0 [no symptoms] to 6 [death]). The primary safety outcomes included mortality at 90 days and the incidence of symptomatic intracranial hemorrhage within 48 hours.
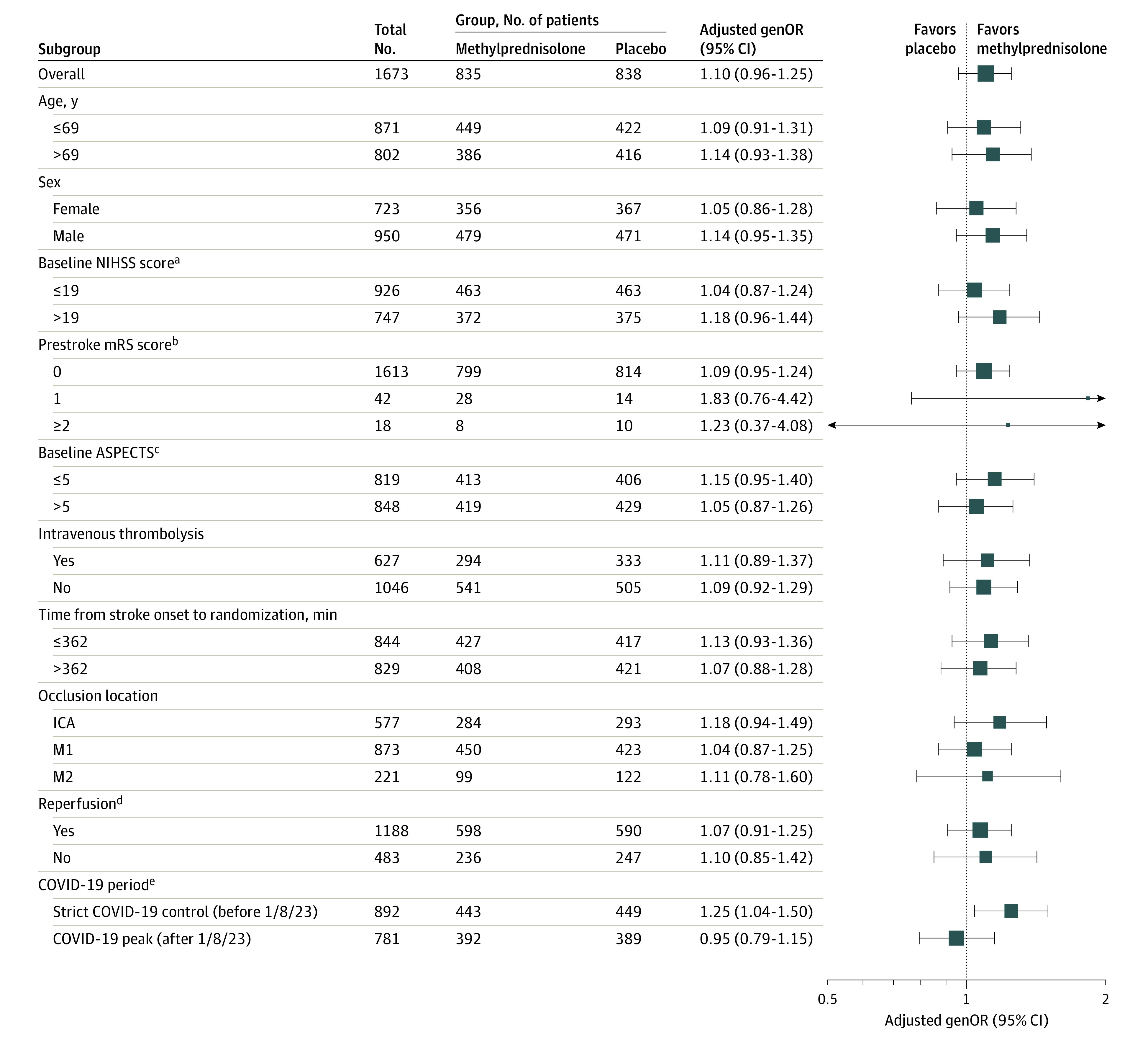
Results: Among 1680 patients randomized (median age, 69 years; 727 female [43.3%]), 1673 (99.6%) completed the trial. The median 90-day modified Rankin Scale score was 3 (IQR, 1-5) in the methylprednisolone group vs 3 (IQR, 1-6) in the placebo group (adjusted generalized odds ratio for a lower level of disability, 1.10 [95% CI, 0.96-1.25]; P = .17). In the methylprednisolone group, there was a lower mortality rate (23.2% vs 28.5%; adjusted risk ratio, 0.84 [95% CI, 0.71-0.98]; P = .03) and a lower rate of symptomatic intracranial hemorrhage (8.6% vs 11.7%; adjusted risk ratio, 0.74 [95% CI, 0.55-0.99]; P = .04) compared with placebo.
Conclusions and relevance: Among patients with acute ischemic stroke due to LVO undergoing endovascular thrombectomy, adjunctive methylprednisolone added to endovascular thrombectomy did not significantly improve the degree of overall disability.
Trial registration: ChiCTR.org.cn Identifier: ChiCTR2100051729.
Conflict of interest statement
Figures
Comment in
-
Adjunctive Steroids as Stroke Reperfusion Strategy.JAMA. 2024 Mar 12;331(10):829-830. doi: 10.1001/jama.2024.0526. JAMA. 2024. PMID: 38329442 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
