

Predictors of lack of response to methotrexate in juvenile idiopathic arthritis associated uveitis
- PMID: 38331409
- PMCID: PMC11781584
- DOI: 10.1093/rheumatology/keae079
Predictors of lack of response to methotrexate in juvenile idiopathic arthritis associated uveitis
Abstract
Objectives: To investigate clinical features associated with lack of response to MTX in juvenile idiopathic arthritis associated uveitis (JIA-U).
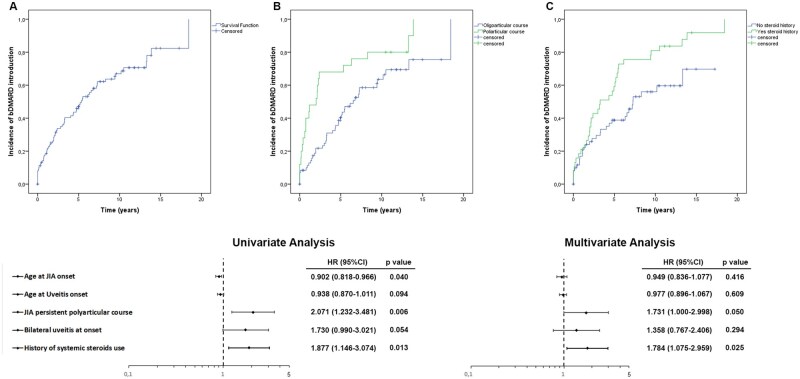
Methods: Clinical records of JIA-U patients were retrospectively reviewed. Differences among variables were assessed by Mann-Whitney and χ2 or Fisher's exact tests as appropriate. Association between predictors and requirement of a biological disease-modifying antirheumatic drug (bDMARD) was evaluated by univariate Cox regression analysis and Kaplan-Meier curves. A multivariable logistic model was applied to estimate strength of association, adjusting for potential confounders.
Results: Data from 99 JIA-U patients treated with MTX were analysed (82.8% female), with a mean follow up of 9.2 years and a mean age at uveitis onset of 5.7 years. In 65 patients (65.7%) at least one bDMARD to control uveitis was required. Children requiring a bDMARD for uveitis had lower age at JIA and uveitis onset, more frequent polyarticular course, higher frequency of bilateral uveitis at onset and higher prevalence of systemic steroids' use. Despite similar frequency of ocular damage at onset, MTX non-responders showed a higher percentage of ocular damage at last visit. Younger age at JIA onset, polyarticular course and a history of systemic steroids' use resulted independent factors associated to lack of response to MTX at Cox regression analysis. Kaplan-Meier curves and the multivariate model confirm the independent role of both polyarticular course and systemic steroids' use.
Conclusions: Younger age at JIA onset, polyarticular course and a history of systemic steroids' use are predictors of a worse response to MTX in JIA-U.
Keywords: biologics; juvenile idiopathic arthritis; methotrexate; uveitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
Comment in
-
Comment on: Predictors of lack of response to methotrexate in juvenile idiopathic arthritis-associated uveitis.Rheumatology (Oxford). 2025 Aug 1;64(8):4862. doi: 10.1093/rheumatology/keaf222. Rheumatology (Oxford). 2025. PMID: 40268864 No abstract available.
References
-
- Petty RE, Rosenbaum JT. Uveitis in juvenile idiopathic arthritis. In: Petty RE, Laxer RM, Lindsley CB, Wedderburn LR, eds. Textbook of pediatric rheumatology. 7th edn. Elsevier (PA; ), 2016: 274–84.
-
- Foeldvari I. Ocular involvement in juvenile idiopathic arthritis: classification and treatment. Clin Rev Allergy Immunol 2015;49:271–7. - PubMed
-
- Tappeiner C, Klotsche J, Schenck S et al. Temporal change in prevalence and complications of uveitis associated with juvenile idiopathic arthritis:data from a cross-sectional analysis of a prospective nationwide study. Clin Exp Rheumatol 2015;33:936–44. - PubMed
-
- Papadopoulou C, Kostik M, Böhm M et al. Methotrexate therapy may prevent the onset of uveitis in juvenile idiopathic arthritis. J Pediatr 2013;163:879–84. - PubMed
