

Polymeric DNase-I nanozymes targeting neutrophil extracellular traps for the treatment of bowel inflammation
- PMID: 38332364
- PMCID: PMC10853102
- DOI: 10.1186/s40580-024-00414-9
Polymeric DNase-I nanozymes targeting neutrophil extracellular traps for the treatment of bowel inflammation
Abstract
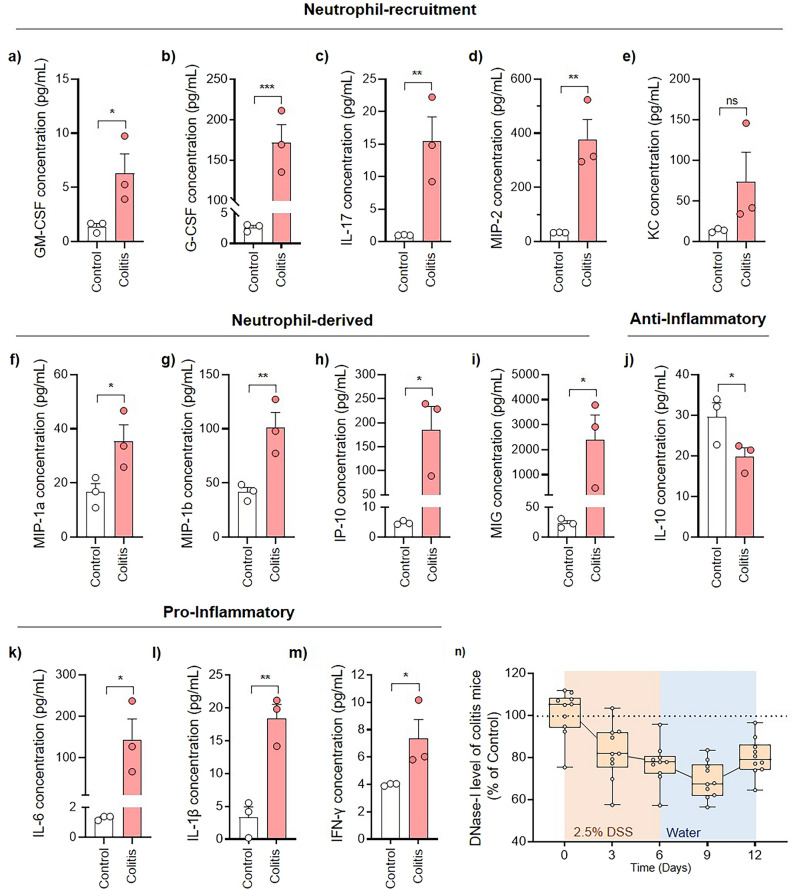
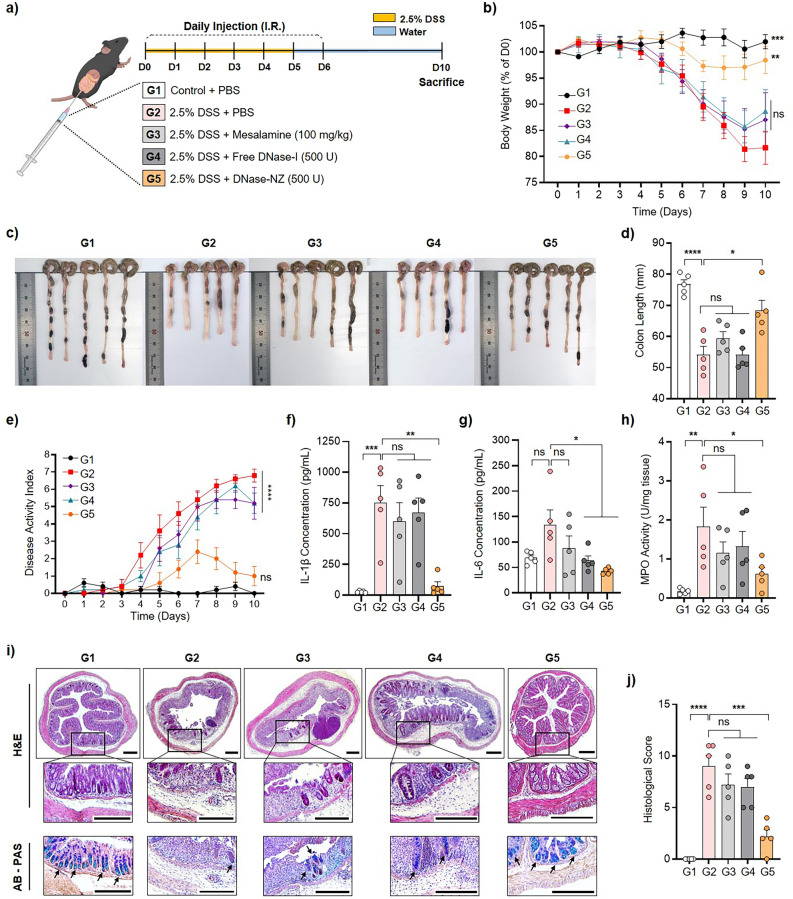
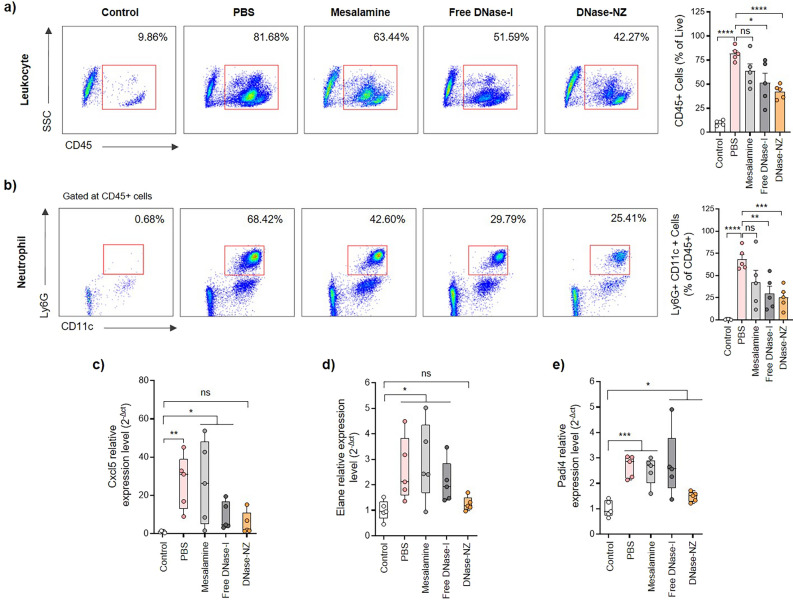
Inflammatory bowel disease (IBD), including Crohn's disease and ulcerative colitis, is a family of chronic disorders along the gastrointestinal tract. Because of its idiopathic nature, IBD does not have a fundamental cure; current available therapies for IBD are limited to prolonged doses of immunomodulatory agents. While these treatments may reduce inflammation, limited therapeutic efficacy, inconsistency across patients, and adverse side effects from aggressive medications remain as major drawbacks. Recently, excessive production and accumulation of neutrophil extracellular traps (NETs) also known as NETosis have been identified to exacerbate inflammatory responses and induce further tissue damage in IBD. Such discovery invited many researchers to investigate NETs as a potential therapeutic target. DNase-I is a natural agent that can effectively destroy NETs and, therefore, potentially reduce NETs-induced inflammations even without the use of aggressive drugs. However, low stability and rapid clearance of DNase-I remain as major limitations for further therapeutic applications. In this research, polymeric nanozymes were fabricated to increase the delivery and therapeutic efficacy of DNase-I. DNase-I was immobilized on the surface of polymeric nanoparticles to maintain its enzymatic properties while extending its activity in the colon. Delivery of DNase-I using this platform allowed enhanced stability and prolonged activity of DNase-I with minimal toxicity. When administered to animal models of IBD, DNase-I nanozymes successfully alleviated various pathophysiological symptoms of IBD. More importantly, DNase-I nanozyme administration successfully attenuated neutrophil infiltration and NETosis in the colon compared to free DNase-I or mesalamine.
Keywords: Colitis; DNase-I; Inflammatory bowel disease; Nanoparticle; Neutrophil extracellular trap.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Neutrophil Extracellular Traps Induce Intestinal Damage and Thrombotic Tendency in Inflammatory Bowel Disease.J Crohns Colitis. 2020 Feb 10;14(2):240-253. doi: 10.1093/ecco-jcc/jjz132. J Crohns Colitis. 2020. PMID: 31325355
-
DNase aggravates intestinal microvascular injury in IBD patients by releasing NET-related proteins.FASEB J. 2024 Jan;38(1):e23395. doi: 10.1096/fj.202301780R. FASEB J. 2024. PMID: 38149880
-
Neutrophil extracellular traps in inflammatory bowel diseases: Implications in pathogenesis and therapeutic targets.Pharmacol Res. 2021 Sep;171:105779. doi: 10.1016/j.phrs.2021.105779. Epub 2021 Jul 21. Pharmacol Res. 2021. PMID: 34298111 Review.
-
Unraveling the intricacies of neutrophil extracellular traps in inflammatory bowel disease: Pathways, biomarkers, and promising therapies.Cytokine Growth Factor Rev. 2024 Dec;80:156-167. doi: 10.1016/j.cytogfr.2024.10.003. Epub 2024 Oct 18. Cytokine Growth Factor Rev. 2024. PMID: 39438227 Review.
-
Neutrophil extracellular traps in pediatric inflammatory bowel disease.Pathol Int. 2018 Sep;68(9):517-523. doi: 10.1111/pin.12715. Epub 2018 Aug 22. Pathol Int. 2018. PMID: 30133056
Cited by
-
Classification of Nanomaterial Drug Delivery Systems for Inflammatory Bowel Disease.Int J Nanomedicine. 2025 Feb 3;20:1383-1399. doi: 10.2147/IJN.S502546. eCollection 2025. Int J Nanomedicine. 2025. PMID: 39925683 Free PMC article. Review.
-
Lactobacillus johnsonii alleviates experimental colitis by restoring intestinal barrier function and reducing NET-mediated gut-liver inflammation.Commun Biol. 2025 Aug 14;8(1):1222. doi: 10.1038/s42003-025-08679-4. Commun Biol. 2025. PMID: 40813467 Free PMC article.
-
Neutrophils at the Crossroads of Inflammatory Bowel Disease and Atherosclerosis: A State-of-the-Art Review.Cells. 2025 May 18;14(10):738. doi: 10.3390/cells14100738. Cells. 2025. PMID: 40422241 Free PMC article. Review.
-
Neutrophils and NETs in Pathophysiology and Treatment of Inflammatory Bowel Disease.Int J Mol Sci. 2025 Jul 23;26(15):7098. doi: 10.3390/ijms26157098. Int J Mol Sci. 2025. PMID: 40806230 Free PMC article. Review.
-
Innovative nanoparticle-based approaches for modulating neutrophil extracellular traps in diseases: from mechanisms to therapeutics.J Nanobiotechnology. 2025 Feb 6;23(1):88. doi: 10.1186/s12951-025-03195-3. J Nanobiotechnology. 2025. PMID: 39915767 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources