

Management of Hypertension in the Asia-Pacific Region: A Structured Review
- PMID: 38332411
- PMCID: PMC10973088
- DOI: 10.1007/s40256-023-00625-1
Management of Hypertension in the Asia-Pacific Region: A Structured Review
Abstract
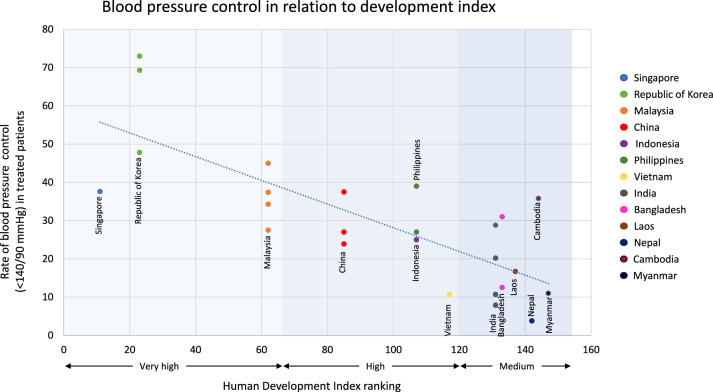
This article reviews available evidence regarding hypertension management in the Asia-Pacific region, focussing on five research questions that deal with specific aspects: blood pressure (BP) control, guideline recommendations, role of renin-angiotensin-aldosterone system (RAAS) inhibitors in clinical practice, pharmacological management and real-world adherence to guideline recommendations. A PubMed search identified 2537 articles, of which 94 were considered relevant. Compared with Europeans, Asians have higher systolic/diastolic/mean arterial BP, with a stronger association between BP and stroke. Calcium channel blockers are the most-commonly prescribed monotherapy in Asia, with significant variability between countries in the rates of angiotensin-converting enzyme inhibitors (ACEis)/angiotensin-receptor blockers (ARBs) and single-pill combination (SPC) use. In clinical practice, ARBs are used more commonly than ACEis, despite the absence of recommendation from guidelines and clinical evidence supporting the use of one class of drug over the other. Ideally, antihypertensive treatment should be tailored to the individual patient, but currently there are limited data on the characteristics of hypertension in Asia-Pacific individuals. Large outcome studies assessing RAAS inhibitor efficacy and safety in multi-national Asian populations are lacking. Among treated patients, BP control rates were ~ 35 to 40%; BP control in Asia-Pacific is suboptimal, and disproportionately so compared with Western nations. Strategies to improve the management of hypertension include wider access/availability of affordable treatments, particularly SPCs (which improve adherence), effective public health screening programs targeting patients to drive health-seeking behaviours, an increase in physician/patient awareness and early implementation of lifestyle changes. A unified Asia-Pacific guideline on hypertension management with pragmatic recommendations, particularly in resource-limited settings, is essential.
© 2024. The Author(s).
Conflict of interest statement
AR has received honoraria as a speaker for several pharmaceutical companies; has been engaged and paid as Advisory Board Member of several companies; has received lecture honoraria from Servier, Novartis, Sanofi, Viatris and Duopharma; and has received advisory board honoraria from Novartis and Sanofi. JDAM has received honoraria for previous CME engagements on hypertension with Merck, Servier and Torrent. JC has received honoraria for presentations and involvement in educational seminars from Servier, Merck and Norva. MH has received honoraria for presentations and involvement in educational seminars from Servier. H-YL has received honoraria for presentations and involvement in educational seminars from Servier, AstraZeneca, Daichi Sankyo, Daewoong, Boryung and Novartis. TN has received an honorarium from Servier for educational events/presentations. ON has received honoraria for presentations and involvement in educational seminars from Servier, AstraZeneca and Novartis. JP has received honoraria for presentations and involvement in educational seminars from Servier, AstraZeneca, Boehringer Ingelheim, Pfizer, Daiichi Sankyo, Bayer, Novo Nordisk, Amgen, Sanofi and Novartis. HVM has received honoraria for presentations and involvement in educational seminars from Servier, AstraZeneca and Novartis. RK has received honoraria for presentations and involvement in educational seminars from Servier, Merck and Boehringer-Ingelheim.
Figures

References
-
- The World Bank. Population, total. 2021. https://data.worldbank.org/indicator/SP.POP.TOTL. Accessed 29 Sept 2022.
-
- World Health Organization. Noncommunicable diseases. 2022. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. Accessed 30 Sept 2022.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
