

Bundling Colorectal Cancer Screening Outreach with Screening for Social Risk in Federally Qualified Health Centers: A Stepped-Wedge Implementation-Effectiveness Study
- PMID: 38332440
- PMCID: PMC11116362
- DOI: 10.1007/s11606-024-08654-5
Bundling Colorectal Cancer Screening Outreach with Screening for Social Risk in Federally Qualified Health Centers: A Stepped-Wedge Implementation-Effectiveness Study
Abstract
Background: Bundling is combining individual interventions to meet quality metrics. Bundling offers of cancer screening with screening for social determinants of health (SDOH) may enable health centers to assist patients with social risks and yield efficiencies.
Objective: To measure effects of bundling fecal immunochemical testing (FIT) and SDOH screening in federally qualified health centers (FQHCs).
Design: Clustered stepped-wedge trial.
Participants: Four Massachusetts FQHCs randomized to implement bundled FIT-SDOH over 8-week "steps."
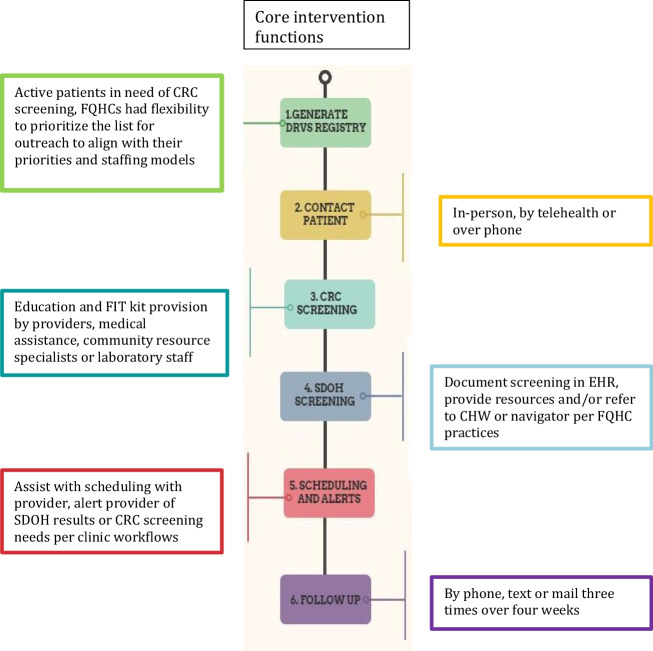
Intervention: Outreach to 50-75-year-olds overdue for CRC screening to offer FIT with SDOH screening. The implementation strategy used facilitation and training for data monitoring and reporting.
Main measures: Implementation process descriptions, data from facilitation meetings, and CRC and SDOH screening rates. Rates were compared between implementation and control FQHCs in each "step" by fitting generalized linear mixed-effects models with random intercepts for FQHCs, patients, and "step" by FQHC.
Key results: FQHCs tailored implementation processes to their infrastructure, workflows, and staffing and prioritized different groups for outreach. Two FQHCs used population health outreach, and two integrated FIT-SDOH within established programs, such as pre-visit planning. Of 34,588 patients overdue for CRC screening, 54% were female; 20% Black, 11% Latino, 10% Asian, and 47% white; 32% had Medicaid, 16% Medicare, 32% private insurance, and 11% uninsured. Odds of CRC screening completion in implementation "steps" compared to controls were higher overall and among groups prioritized for outreach (overall: adjusted odds ratio (aOR) 2.41, p = 0.005; prioritized: aOR 2.88, p = 0.002). Odds of SDOH screening did not differ across "steps."
Conclusions: As healthcare systems are required to conduct more screenings, it is notable that outreach for a long-standing cancer screening requirement increased screening, even when bundled with a newer screening requirement. This outreach was feasible in a real-world safety-net clinical population and may conserve resources, especially compared to more complex or intensive outreach strategies.
Clinical trials registration: NCT04585919.
Keywords: colorectal cancer; community health centers; implementation science.; screening; social determinants of health.
© 2024. The Author(s).
Conflict of interest statement
GK has a family financial interest in Dimagi, Inc., and received a research grant from the National Comprehensive Cancer Network/Astra Zeneca. All other authors have no conflicts of interest to declare.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
