

Current role of intraoperative cell salvage techniques in the management of renal tumors with level III and IV inferior vena cava thrombus extension
- PMID: 38333071
- PMCID: PMC10851714
- DOI: 10.1177/17562872241229248
Current role of intraoperative cell salvage techniques in the management of renal tumors with level III and IV inferior vena cava thrombus extension
Abstract
Background: En bloc removal of the kidney with tumor thrombus excision in a multidisciplinary team remains the standard treatment for renal cell carcinoma (RCC) with tumor thrombus extension. In order to minimize the hemodynamic impact of the surgical blood loss, intraoperative cell salvage (IOCS) techniques can decrease the need for allogeneic blood and prevent blood transfusion related complications.
Objective: In this article, we evaluated the safety of IOCS during radical nephrectomy with inferior vena cava thrombectomy under cardiopulmonary bypass with or without deep hypothermic circulatory arrest.
Design and method: In this retrospective comparative multicenter analysis, clinical characteristics of 27 consecutive patients who underwent surgery with or without IOCS between 2012 and 2022 in three referral care units were collected into a database. The need for an allogenic blood transfusion (ABT) was also recorded, defined as any transfusion that occurred either intraoperatively or during the hospital stay.
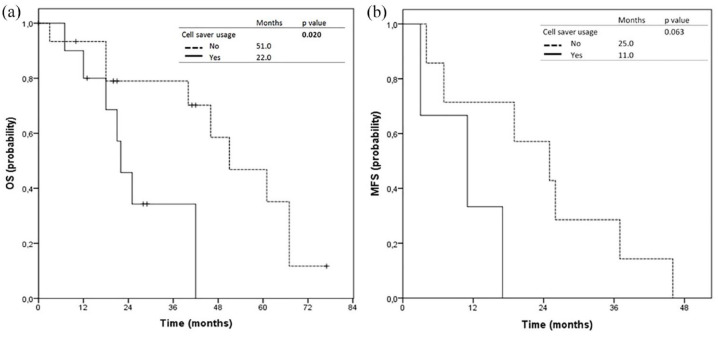
Results: The need for ABT in the cell saver arm was significantly smaller due to the reinfusion of rescued blood (p < 0.015). In multivariate analysis, no cell saver usage was an independent predictor for complications ⩾3 Clavien 3a [odds ratio (OR) 18.71, 95% CI 1.056-331.703, p = 0.046]. No usage of IOCS was an independent predictor for a lower risk of death (OR 0.277, 95% CI 0.062-0.825, p = 0.024). During follow-up, patients who received salvaged blood did not experience an increased risk for developing local recurrence or distant metastases.
Conclusion: Transfusion of autologous blood is safe and can be using during nephrectomy and thrombectomy for advanced RCC.
Keywords: advanced renal cell carcinoma; blood management; cavoatrial extension; intraoperative cell salvage techniques; oncological outcomes.
Plain language summary
Role of intraoperative cell salvage techniques in the management of renal tumors with advanced caval extension En bloc removal of the kidney with tumor thrombus excision in a multidisciplinary team remains the standard treatment for RCC with tumor thrombus extension. Intraoperative cell salvage techniques (IOCS) can decrease the need for allogeneic blood and prevent blood transfusion related complications. In this article we demonstrated that transfusion of autologous blood is safe and can be using during nephrectomy and thrombectomy for advanced renal cell carcinoma.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
[Application of intraoperative cell salvage combined with leukocyte depletion filter on radical nephrectomy for renal carcinoma with inferior vena cava tumor thrombus: 2 case reports].Beijing Da Xue Xue Bao Yi Xue Ban. 2017 Aug 18;49(4):736-739. Beijing Da Xue Xue Bao Yi Xue Ban. 2017. PMID: 28816299 Chinese.
-
Retrohepatic inferior vena cava control through an anterior approach in cases of renal cell carcinoma with level IIIa tumor thrombus: Step-by-step description.Actas Urol Esp (Engl Ed). 2021 Nov;45(9):587-596. doi: 10.1016/j.acuroe.2021.04.012. Epub 2021 Oct 23. Actas Urol Esp (Engl Ed). 2021. PMID: 34697007 English, Spanish.
-
Treatment of renal cell carcinoma with a level III or level IV inferior vena cava thrombus using cardiopulmonary bypass and deep hypothermic circulatory arrest.World J Surg Oncol. 2015 Apr 22;13:159. doi: 10.1186/s12957-015-0584-8. World J Surg Oncol. 2015. PMID: 25897659 Free PMC article.
-
Important surgical considerations in the management of renal cell carcinoma (RCC) with inferior vena cava (IVC) tumour thrombus.BJU Int. 2012 Oct;110(7):926-39. doi: 10.1111/j.1464-410X.2012.11174.x. Epub 2012 Apr 30. BJU Int. 2012. PMID: 22540179 Review.
-
Surgical treatment of renal cell carcinoma with inferior vena cava tumor thrombus.Surg Today. 2022 Aug;52(8):1125-1133. doi: 10.1007/s00595-021-02429-9. Epub 2022 Jan 3. Surg Today. 2022. PMID: 34977987 Review.
References
-
- Ljungberg B, Albiges L, Abu-Ghanem Y, et al.. European association of urology guidelines on renal cell carcinoma: the 2022 update. Eur Urol 2022; 82: 399–410. - PubMed
-
- Blute ML, Leibovich BC, Lohse CM, et al.. The Mayo clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU Int 2004; 94: 33–41. - PubMed
-
- Wotkowicz C, Libertino JA, Sorcini A, et al.. Management of renal cell carcinoma with vena cava and atrial thrombus: minimal access vs median sternotomy with circulatory arrest. BJU Int 2006; 98: 289–297. - PubMed
-
- Kirkali Z, Van Poppel H. A critical analysis of surgery for kidney cancer with vena cava invasion. Eur Urol 2007; 52: 658–662. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
