

Critical care of severe bronchiolitis during shortage of ICU resources
- PMID: 38333363
- PMCID: PMC10850123
- DOI: 10.1016/j.eclinm.2024.102450
Critical care of severe bronchiolitis during shortage of ICU resources
Abstract
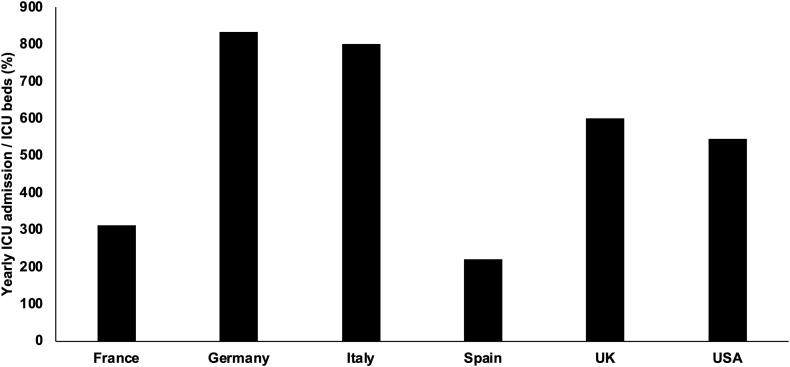
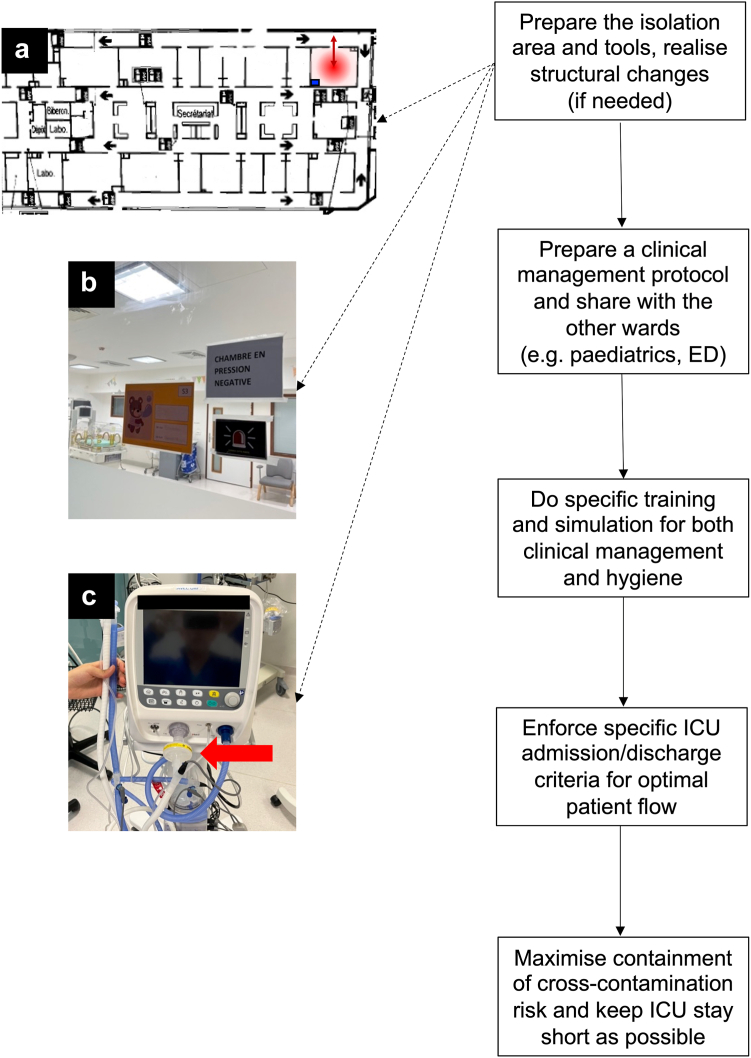
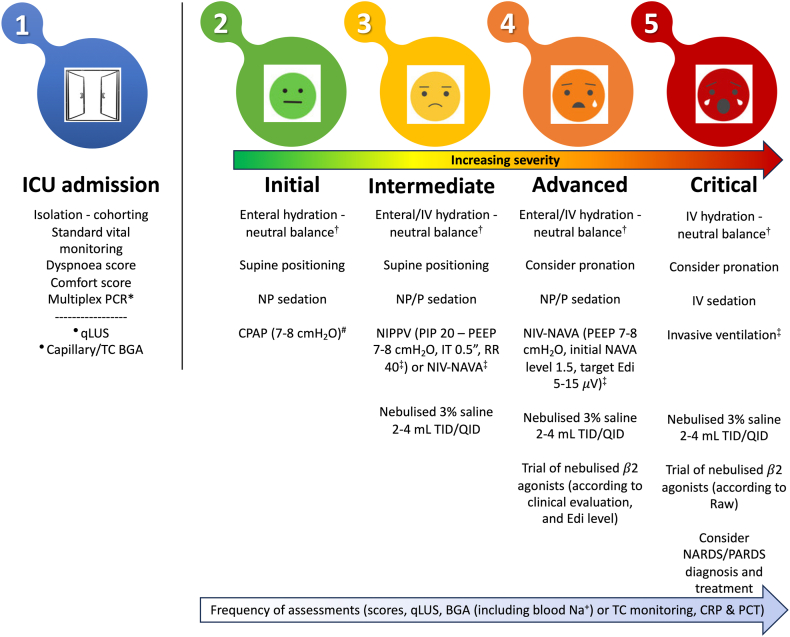
Large seasonal outbreaks of bronchiolitis put pressure on healthcare systems and particularly on intensive care units (ICUs). ICU admission is necessary to provide respiratory support to the severest cases, otherwise bronchiolitis can result in substantial mortality. ICU resources are often insufficient and there is scant evidence to guide the ICU clinical management. Most available studies do not cover the ICU-admitted cases and do not consider the associated public health issues. We review this topic through a multidisciplinary approach from both the clinical and public health perspectives, with an analysis based on pathophysiology and cost-effectiveness. We suggest ways to optimise respiratory care, minimise ICU stay, "protect" ICU beds and, whenever possible, make them available for other critically ill children. We also provide guidance on how to prepare ICUs to work under stressful conditions due to outbreaks and to reduce the risk of nosocomial cross-contamination, particularly in ICUs caring for high-risk children.
Funding: None.
Keywords: Infant; NICU; Outbreak; PICU; RSV; Respiratory failure.
© 2024 The Author(s).
Conflict of interest statement
DDL has received lecture fees or research and educational support or from Chiesi Farmaceutici, Getinge, Vyaire, Radiometer, Medtronic, AstraZeneca, Boehringer Ingelheim, Airway Therapeutics, Natus, Masimo and BD. He has equity options from Ophirex ltd; he also participated to a data safety monitoring board for EXO biologics. All these were unrelated to this work and the field of bronchiolitis in general; finally, he is the Immediate Past President of the European Society for Paediatric and Neonatal Intensive Care (ESPNIC). MDN participated to the medical advisory board of Eurosets, unrelated to this work and the field of bronchiolitis in general; he is also the Secretary of ESPNIC. EB has received consultancy and lecture fees and has participated in advisory boards for AstraZeneca and Sanofi, all outside of the present work. MRG received a lecture fee from Sanofi, unrelated to this work and the field of bronchiolitis in general. The other authors have no interest to declare. This work did not receive any funding.
Figures
References
-
- Cohen C., Zar H.J. Deaths from RSV in young infants—the hidden community burden. Lancet Glob Health. 2022;10:e169–e170. - PubMed
-
- Pierce H., Mansbach J., Fisher E., et al. Variability of intensive care management for children with bronchiolitis. Hosp Pediatr. 2015;5:174–184. - PubMed
-
- Milési C., Baudin F., Durand P., et al. Clinical practice guidelines: management of severe bronchiolitis in infants under 12 months old admitted to a pediatric critical care unit. Intensive Care Med. 2023;49:5–25. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
