

Dabrafenib and trametinib administration in patients with BRAF V600E/R or non-V600 BRAF mutated advanced solid tumours (BELIEVE, NCCH1901): a multicentre, open-label, and single-arm phase II trial
- PMID: 38333370
- PMCID: PMC10850114
- DOI: 10.1016/j.eclinm.2024.102447
Dabrafenib and trametinib administration in patients with BRAF V600E/R or non-V600 BRAF mutated advanced solid tumours (BELIEVE, NCCH1901): a multicentre, open-label, and single-arm phase II trial
Abstract
Background: BRAF V600 mutations are common in melanoma, thyroid, and non-small-cell lung cancers. Despite dabrafenib and trametinib being standard treatments for certain cancers, their efficacy across various solid tumours remains unelucidated. The BELIEVE trial assessed the efficacy of dabrafenib and trametinib in solid tumours with BRAF V600E/R or non-V600 BRAF mutations.
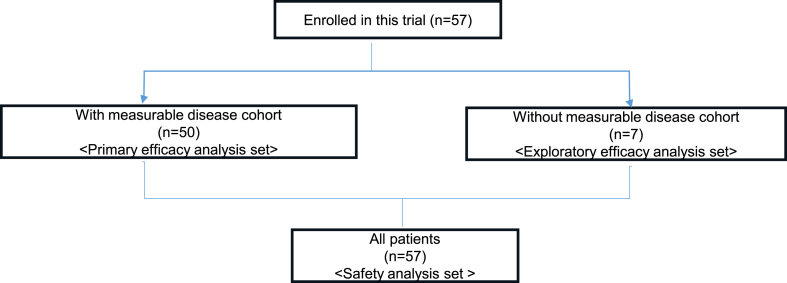
Methods: Between October 1, 2019, and June 2022, at least 50 patients with measurable and seven without measurable diseases examined were enrolled in a subcohort of the BELIEVE trial (NCCH1901, jRCTs031190104). BRAF mutated solid tumour cases other than BRAF V600E mutated colorectal cancer, melanoma, and non-small cell lung cancer cases were included. Patients with solid tumours received dabrafenib (150 mg) twice daily and trametinib (2 mg) once daily until disease progression or intolerable toxicity was observed. The primary endpoint was overall response rate (ORR), and secondary endpoints included progression-free survival (PFS), 6-month PFS, and overall survival (OS). Bayesian analysis was performed using a prior distribution with a 30% expected response rate [Beta (0.6, 1.4)].
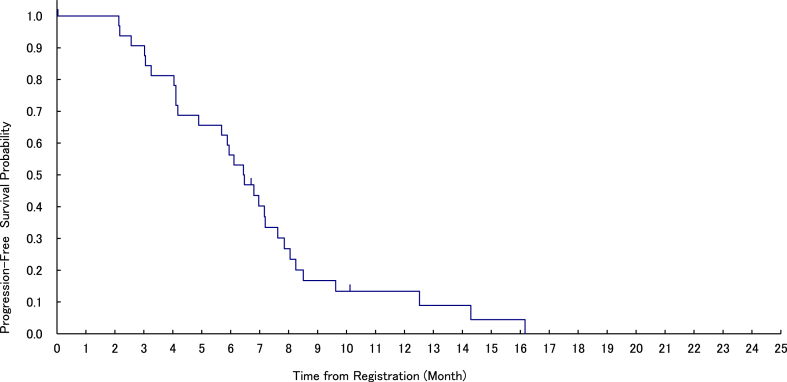
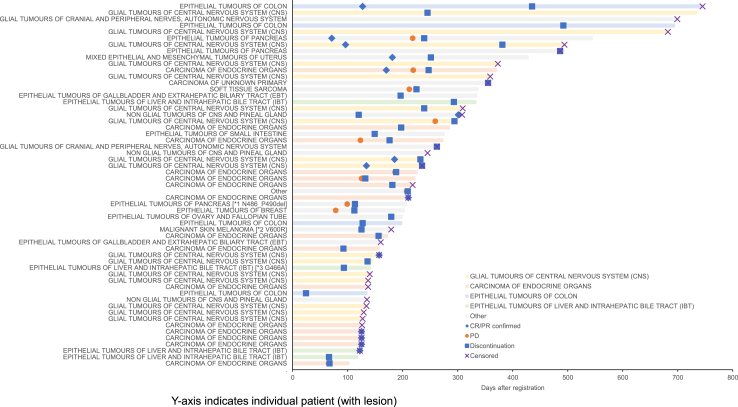
Findings: Fourty-seven patients with measurable disease, mainly with the BRAF V600E mutation (94%), and three others with non-V600E BRAF mutations (V600R, G466A, and N486_P490del) were enrolled. The primary sites included the thyroid gland, central nervous system, liver, bile ducts, colorectum, and pancreas. The confirmed ORR was 28.0%; the expected value of posterior distribution [Beta (14.6, 37.4)] was 28.1%, although the primary endpoint was achieved, not exceeding an unexpectedly high response rate of 60% obtained using Bayesian analysis. The disease control rate (DCR) was 84.0%. The median PFS was 6.5 months (95% confidence interval [CI]; 4.2-7.2 months, 87.8% at 6 months). Responses were observed across seven tumour types. Median OS was 9.7 months (95% CI, 7.5-12.2 months). Additional patients without measurable diseases had a median PFS of 4.5 months. Adverse events (AEs) were consistent with previous reports, with 45.6% of patients experiencing grade ≥3 AEs.
Interpretation: This study reported promising efficacy against BRAF V600-mutant tumours. Dabrafenib and trametinib would offer a new therapeutic option for rare cancers, such as high-grade gliomas, biliary tract cancer, and thyroid cancer.
Funding: This study was funded by the Japan Agency for Medical Research and Development (22ck0106622h0003) and a Health and Labour Sciences Research Grant (19EA1008).
Keywords: BRAF inhibitors; Bayesian statistics; MEK inhibitors; Platform clinical trials; Rare cancers.
© 2024 The Author(s).
Conflict of interest statement
Dr. Tahara reports personal fees from Novartis, during the conduct of the study; grants and personal fees from Ono Pharmaceutical, grants and personal fees from Bayer, personal fees from MSD, personal fees from BMS, personal fees from Merck Biopharma, personal fees from Pfizer, personal fees from Rakuten Medical, personal fees from Lilly, personal fees from Boehringer Ingelheim, personal fees from Eisai, personal fees from Chugai Pharmaceutical, personal fees from Daiichi-Sankyo, personal fees from Janssen Pharmaceutical, personal fees from Genmab, personal fees from Astra Zeneca, personal fees from Abbvie, personal fees from Astellas, outside the submitted work. Dr. Yamamoto reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Ono Pharmaceutical, Chugai, Daiichi-Sankyo, Eisai, Payment for expert testimony from Eisai, Takeda, Boehringer Ingelheim, Cimic, Chugai, Other financial or non-financial interests from Astellas, Chugai, Eisai, Taiho, BMS, Pfizer, Novartis, Eli Lilly, AbbVie, Daiichi-Sankyo, Bayer, Boehringer Ingelheim, Kyowa-Hakko Kirin, Takeda, ONO, Janssen Pharma, MSD, MERCK, GSK, Sumitomo Dainippon, Chiome Bioscience, Otsuka, Carna Biosciences, Genmab, Shionogi, TORAY, KAKEN, InventisBio, Rakuten Medical.
Figures
References
-
- Chan A.K., Zhang R.R., Aibaidula A., et al. BRAF mutation marks out specific subgroups of glioma. Glioma. 2018;1:168–174. doi: 10.4103/glioma.glioma_33_18. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
