

Effects of sigmoidoscopy screening (including colonoscopy) on colorectal cancer: A meta-analysis based on randomized controlled trials
- PMID: 38333601
- PMCID: PMC10847765
- DOI: 10.1016/j.pmedr.2024.102636
Effects of sigmoidoscopy screening (including colonoscopy) on colorectal cancer: A meta-analysis based on randomized controlled trials
Abstract
Background: This study aimed to investigate the role of endoscopy screening in colorectal cancer (CRC).
Methods: Up to January 2023, databases were searched for studies related to sigmoidoscopy and colonoscopy screening. The incidence of CRC, and/or CRC mortality were the main observation outcomes.
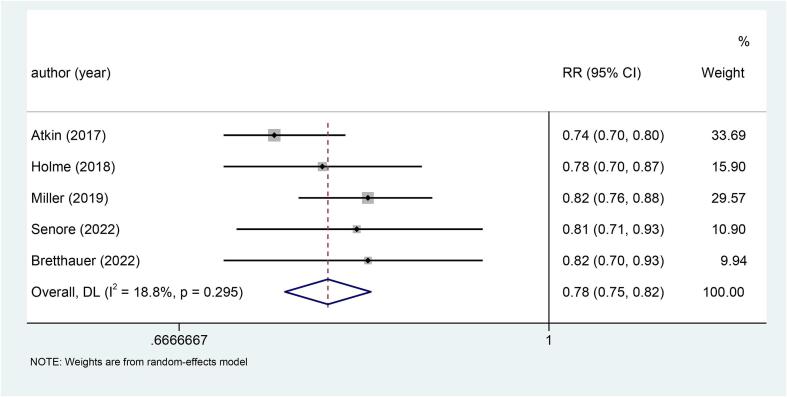
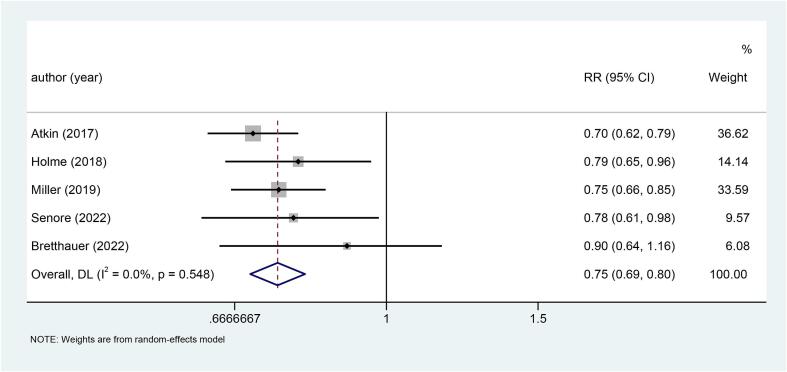
Results: A total of 5 randomized controlled trials (RCTs) published from 2017 to 2022 were included. Among them, four studies used sigmoidoscopy screening and one study involved colonoscopy screening. Statistical results showed that the incidence (RR: 0.78, p < 0.001) and mortality (RR: 0.75, p < 0.001) of CRC were significantly lower in the screening group than in the control group. Further, a subgroup analysis of CRC site indicated that the incidence and mortality of CRC in the screening group were significantly lower than those in the non-screened group, regardless of distal CRC (Incidence: RR: 0.66, p < 0.001; Mortality: RR: 0.62, p < 0.001) or proximal CRC (Incidence: RR: 0.94, p = 0.038; Mortality: RR: 0.89, p = 0.038). In terms of gender, compared with the non-screening group, both males (Incidence: RR: 0.73, p < 0.001; Mortality: RR: 0.68, p < 0.001) and females (Incidence: RR: 0.85, p < 0.001; Mortality: RR: 0.85, p = 0.017), the screening group had a significant decrease in the incidence and mortality of CRC.
Conclusion: This meta-analysis demonstrated that sigmoidoscopy screening (including colonoscopy) could effectively reduce the incidence and mortality of CRC.
Keywords: Colonoscopy; Colorectal Cancer; Incidence; Meta-Analysis; Mortality; Sigmoidoscopy.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures







References
-
- Anderson J.C., et al. Predictors of proximal neoplasia in patients without distal adenomatous pathology. Am. J. Gastroenterol. 2004;99(3):472–477. - PubMed
-
- Arai T., Kino I. Morphometrical and cell kinetic studies of normal human colorectal mucosa. Comparison between the proximal and the distal large intestine. Acta Pathol. Jpn. 1989;39(11):725–730. - PubMed
-
- Atkin W.S., et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375(9726):1624–1633. - PubMed
LinkOut - more resources
Full Text Sources
