

Developments in the Management of Growth Hormone Deficiency: Clinical Utility of Somapacitan
- PMID: 38333899
- PMCID: PMC10849900
- DOI: 10.2147/DDDT.S315172
Developments in the Management of Growth Hormone Deficiency: Clinical Utility of Somapacitan
Abstract
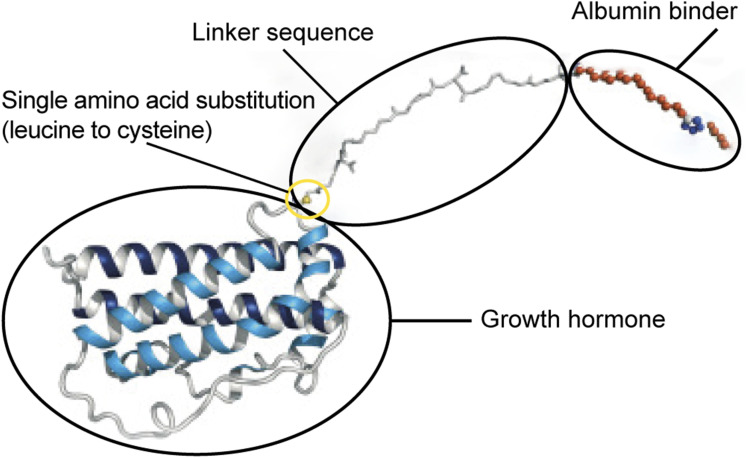
Growth hormone (GH) replacement therapy for growth hormone deficiency (GHD) in children and adults has for over 25 years, until recently, been administered as daily injections. This daily treatment regimen often incurs a burden to patients and caregivers, leading to high rates of non-adherence and, consequently, decreased treatment efficacy outcomes. To address this shortcoming, long-acting growth hormones (LAGHs) have been developed with the aim of reducing the burden of daily injections, thereby potentially improving treatment adherence and outcomes. Somapacitan (Sogroya®) (Novo Nordisk, Bagsværd, Denmark) is a LAGH currently approved for the treatment of adult and childhood GHD (AGHD and CGHD, respectively) in several countries. Other LAGHs, such as somatrogon (Ngenla®) (Pfizer, New York, United States) and lonapegsomatropin/TransCon GH (Skytrofa®) (Ascendis Pharma, Copenhagen, Denmark), are also currently approved and available for the treatment of CGHD in several countries. In this review, we will consider the method of protraction, pharmacokinetics (PK) and pharmacodynamics (PD), efficacy, and safety results of somapacitan in adult and pediatric trials and how these characteristics differ from those of the other aforementioned LAGHs. Additionally, the administration of somapacitan and timing of measurement of serum insulin-like growth factor-I (IGF-I) levels are summarized. Information on administration, advice on missed doses, and clinical guidelines are discussed, as well as identifying which patients are suitable for somapacitan therapy, and how to monitor and adjust dosing whilst on therapy.
Keywords: (3–6): growth hormone; adherence; adult growth hormone deficiency; long-acting growth hormone; pediatric growth hormone deficiency.
© 2024 Miller et al.
Conflict of interest statement
B.S.M.: Consulted for Ascendis Pharma, BioMarin, Bristol Myers Squibb, EMD Serono, Endo Pharmaceuticals, Eton Pharmaceuticals, GenSci, Novo Nordisk, Orchard Therapeutics, Pfizer, Provention Bio, and Tolmar; and received research support from Alexion, AbbVie, Ascendis Pharma, Aeterna Zentaris, Amgen, Amicus, Foresee Pharmaceuticals, Lumos Pharma, Lysogene, Novo Nordisk, OPKO Health, Pfizer, Prevail Therapeutics, and Sangamo Therapeutics. J.B.: Received honoraria for presentations at meetings sponsored by Novo Nordisk, Sandoz, and Ipsen; received sponsorship to attend scientific meetings from Novo Nordisk; and received payment for membership of the Publication Steering Committee of the International Outcomes Study, sponsored by Novo Nordisk. R.H: Advisory board member and lecturer for Novo Nordisk, Pfizer, Lumos Pharma, JCR, and Sandoz. A.L.: Consulted for/received research funding/honoraria from Novo Nordisk, Merck Serono, Alexion, AstraZeneca Rare Disease, and Pfizer Inc; and received honoraria from Ipsen and Sandoz. K.C.J.Y.: Received research grants to Barrow Neurological Institute from Crinetics, Ascendis, Corcept, Amryt, and Sparrow; served as an occasional advisory board member for Novo Nordisk, Ascendis, Ipsen, Amryt, Crinetics, Recordati, Neurocrine, and Xeris; lecture fees from Pfizer; and served as occasional speaker for Recordati and Novo Nordisk.
Figures


References
-
- Miller BS, Rotenstein D, Deeb LC, Germak J, Wisniewski T. Persistence with growth hormone therapy in pediatric patients. Am J Pharm Benefits. 2014;6(1):e9–e17.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
