

Respiratory impairments in patients suffering from Fabry disease - A cross-sectional study
- PMID: 38334083
- PMCID: PMC10858660
- DOI: 10.1177/14799731231221821
Respiratory impairments in patients suffering from Fabry disease - A cross-sectional study
Abstract
Background: The inherited X-linked disorder, Fabry disease, is caused by deficient lysosomal enzyme α-galactosidase A, with progressive accumulation of globotriaosylceramide in multiple organs including the upper and lower airways.
Objectives: To assess pulmonary function at the time of the first pulmonary function test (PFT) performed among the National Danish Fabry cohort and define the prevalence of affected lung function variables.
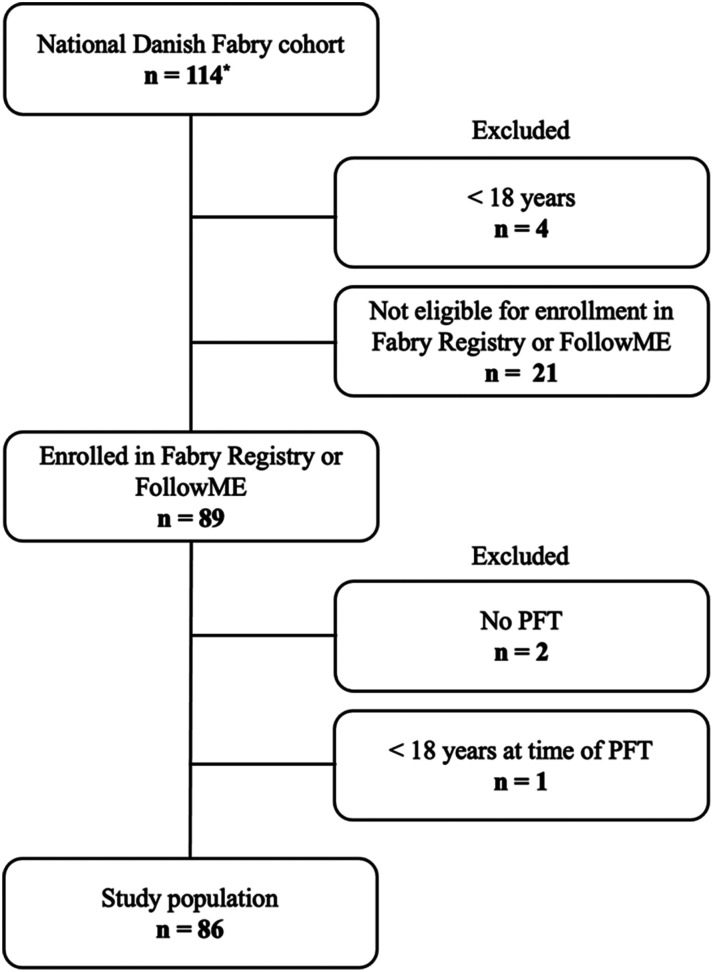
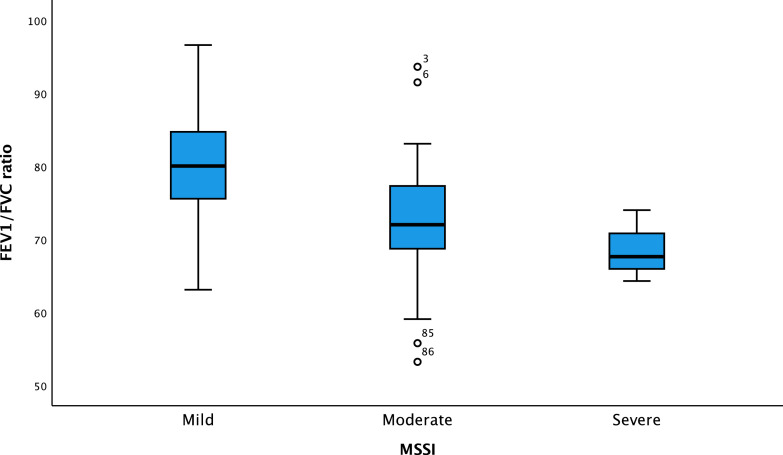
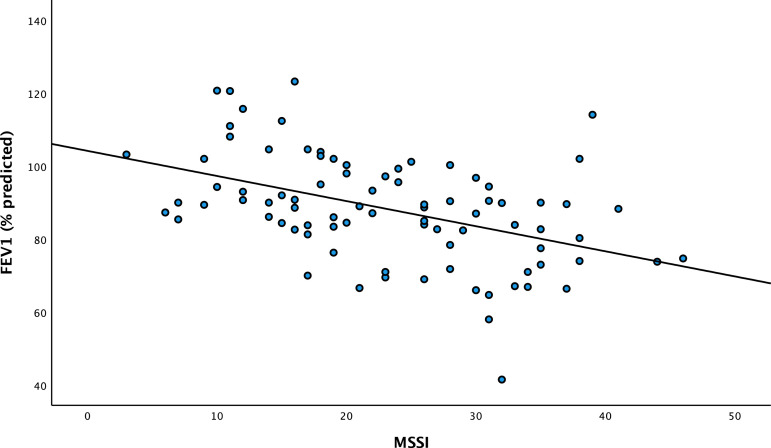
Materials and method: A cross-sectional retrospective cohort study of 86 adult patients enrolled in one or both international patient registry databases for Fabry disease, Fabry Registry or FollowME with at least one PFT. The Mainz Severity Score Index (MSSI) was calculated to determine the disease severity. Lung function variables were examined by multivariate regression adjusted for important variables for developing airway illness.
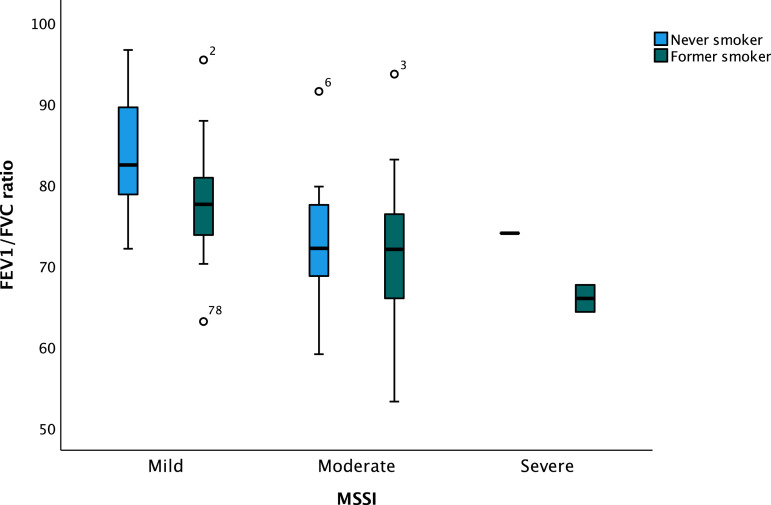
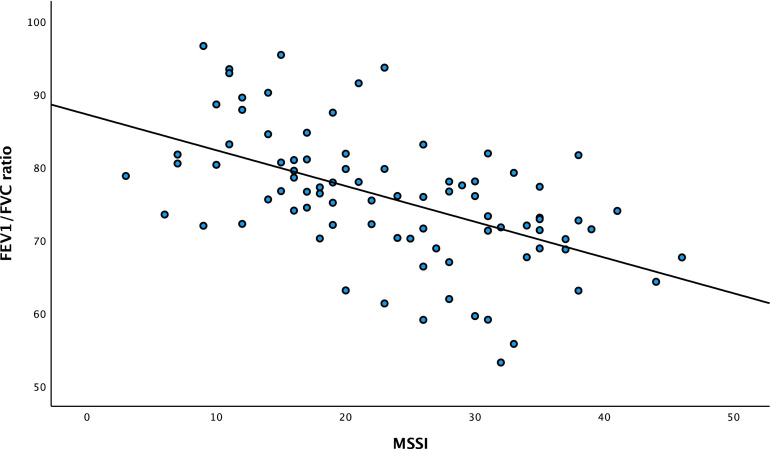
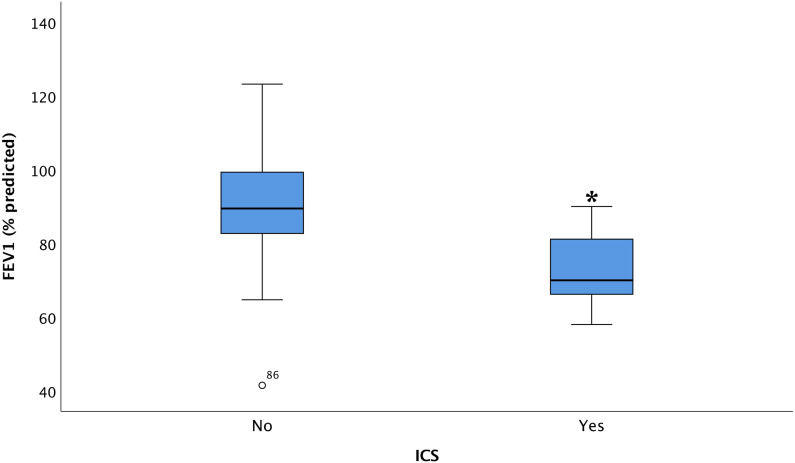
Results: Seventeen patients (20%) showed obstructive airflow limitation and 7 (8%) a restrictive lung deficiency. Smoking status (p = .016) and MSSI (p < .001) were associated with increasing obstructive airway limitation.
Conclusion: The prevalence of affected lung function among the National Danish Fabry cohort was 28%. Patients with classic gene variants frequently developed a decrease in lung function regardless of their smoking status, with significant relationship with disease severity.
Keywords: Fabry disease; pulmonary function test; pulmonary involvement; respiratory impairment.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Bernardes TP, Foresto RD, Kirsztajn GM. Fabry disease: genetics, pathology, and treatment. Rev Assoc Med Bras 2020; 66(Suppl 1): 10–16. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
