

The Role of CCL24 in Primary Sclerosing Cholangitis: Bridging Patient Serum Proteomics to Preclinical Data
- PMID: 38334601
- PMCID: PMC10854794
- DOI: 10.3390/cells13030209
The Role of CCL24 in Primary Sclerosing Cholangitis: Bridging Patient Serum Proteomics to Preclinical Data
Abstract
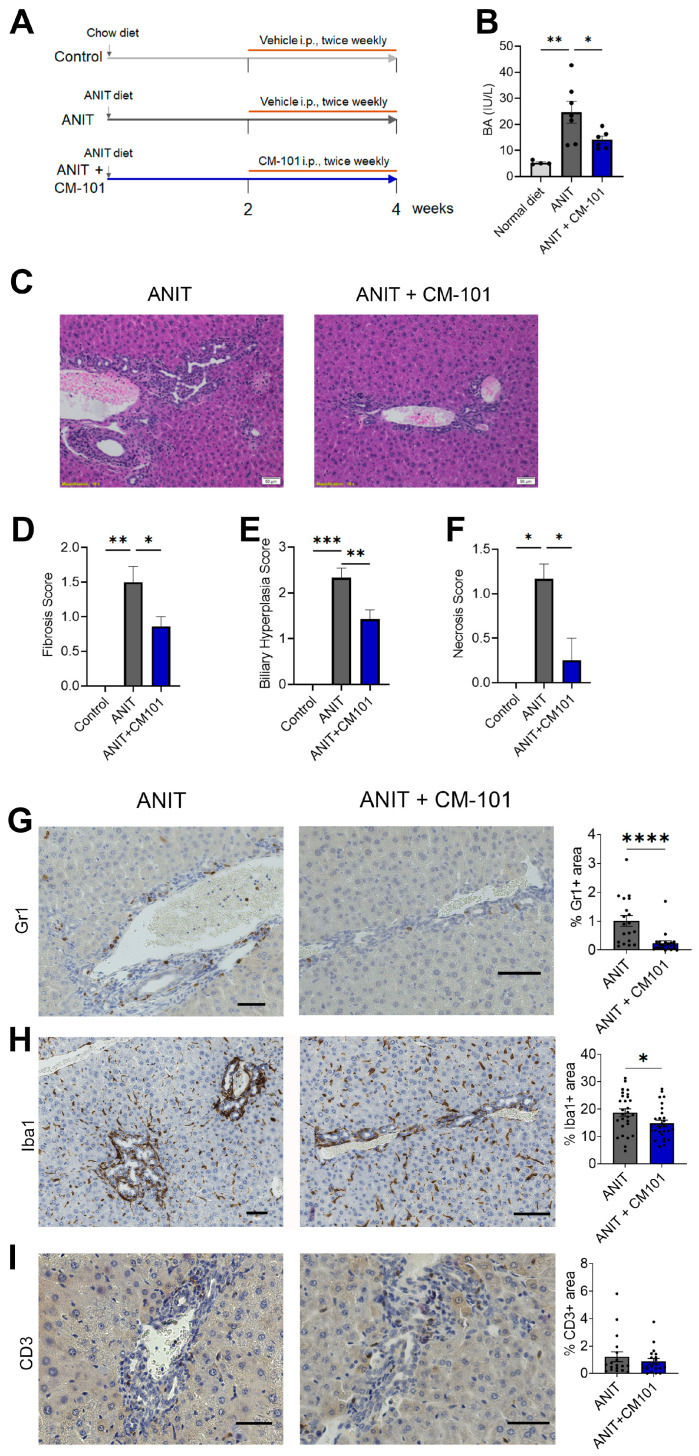
Primary sclerosing cholangitis (PSC) is an inflammatory and fibrotic biliary disease lacking approved treatment. We studied CCL24, a chemokine shown to be overexpressed in damaged bile ducts, and its involvement in key disease-related mechanisms. Serum proteomics of PSC patients and healthy controls (HC) were analyzed using the Olink® proximity extension assay and compared based on disease presence, fibrosis severity, and CCL24 levels. Disease-related canonical pathways, upstream regulators, and toxicity functions were elevated in PSC patients compared to HC and further elevated in patients with high CCL24 levels. In vitro, a protein signature in CCL24-treated hepatic stellate cells (HSCs) differentiated patients by disease severity. In mice, CCL24 intraperitoneal injection selectively recruited neutrophils and monocytes. Treatment with CM-101, a CCL24-neutralizing antibody, in an α-naphthylisothiocyanate (ANIT)-induced cholestasis mouse model effectively inhibited accumulation of peribiliary neutrophils and macrophages while reducing biliary hyperplasia and fibrosis. Furthermore, in PSC patients, CCL24 levels were correlated with upregulation of monocyte and neutrophil chemotaxis pathways. Collectively, these findings highlight the distinct role of CCL24 in PSC, influencing disease-related mechanisms, affecting immune cells trafficking and HSC activation. Its blockade with CM-101 reduces inflammation and fibrosis and positions CCL24 as a promising therapeutic target in PSC.
Keywords: CCL24; chemokines; cholangitis; fibrosis; hepatic stellate cells; inflammation; monocytes; neutrophils; proteomics.
Conflict of interest statement
Avi Katav, Raanan Greenman, Ilan Vaknin, Revital Aricha, Tom Snir, Matthew Frankel, John Lawler, and Adi Mor are employees of Chemomab Therapeutics (Israel). Massimo Pinzani is a Co-Founder and shareholder of Engitix Therapeutics Ltd. (UK), consultant of Chemomab, Chief Medical Advisor and shareholder of Aculive Therapeutics Ltd. (UK), Advisory board/consultant (active March 2022) of Chemomab Therapeutics (Israel); Resolution Therapeutics (UK); Dicerna (USA); Astra Zeneca (UK); and Galecto (Sweden). Amnon Peled is a consultant for Chemomab Therapeutics (Israel). Francesca Saffioti, Douglas Thorburn, Ophir Hay, and Inbal Mishalian have nothing to disclose.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
