

Epidemiology of heart failure in diabetes: a disease in disguise
- PMID: 38334818
- PMCID: PMC10904471
- DOI: 10.1007/s00125-023-06068-2
Epidemiology of heart failure in diabetes: a disease in disguise
Abstract
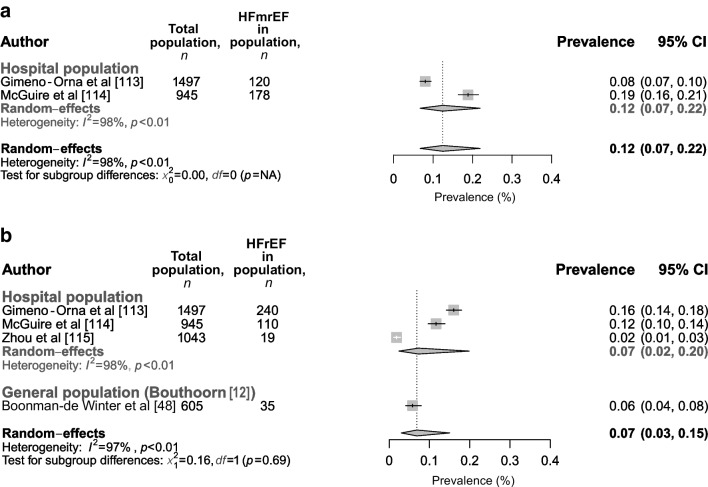
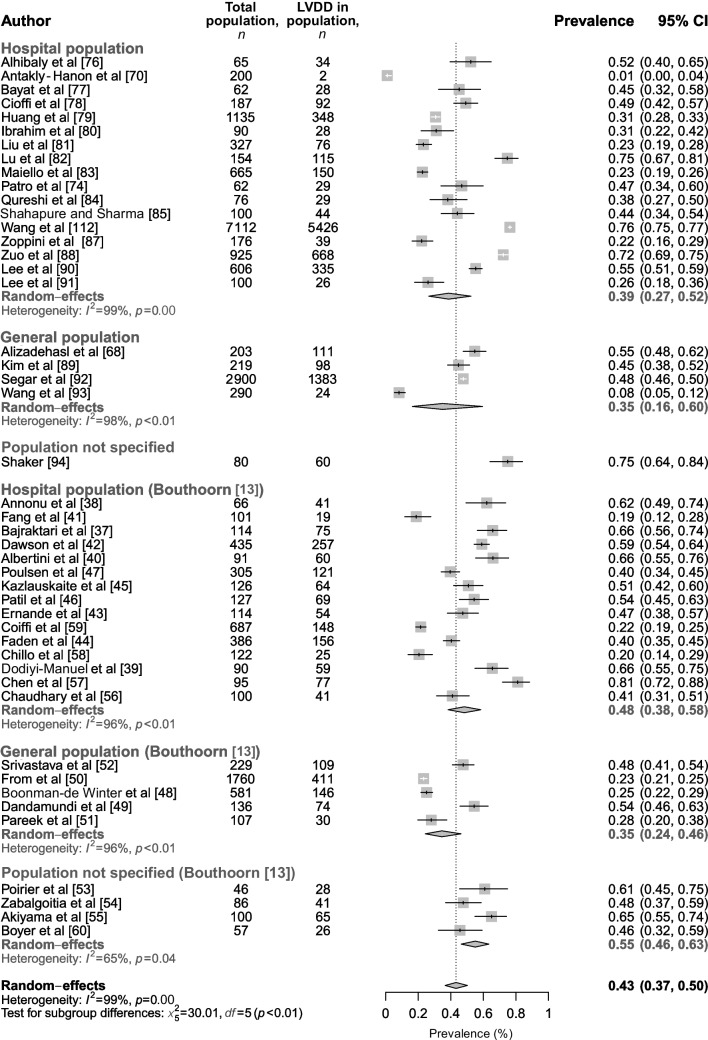
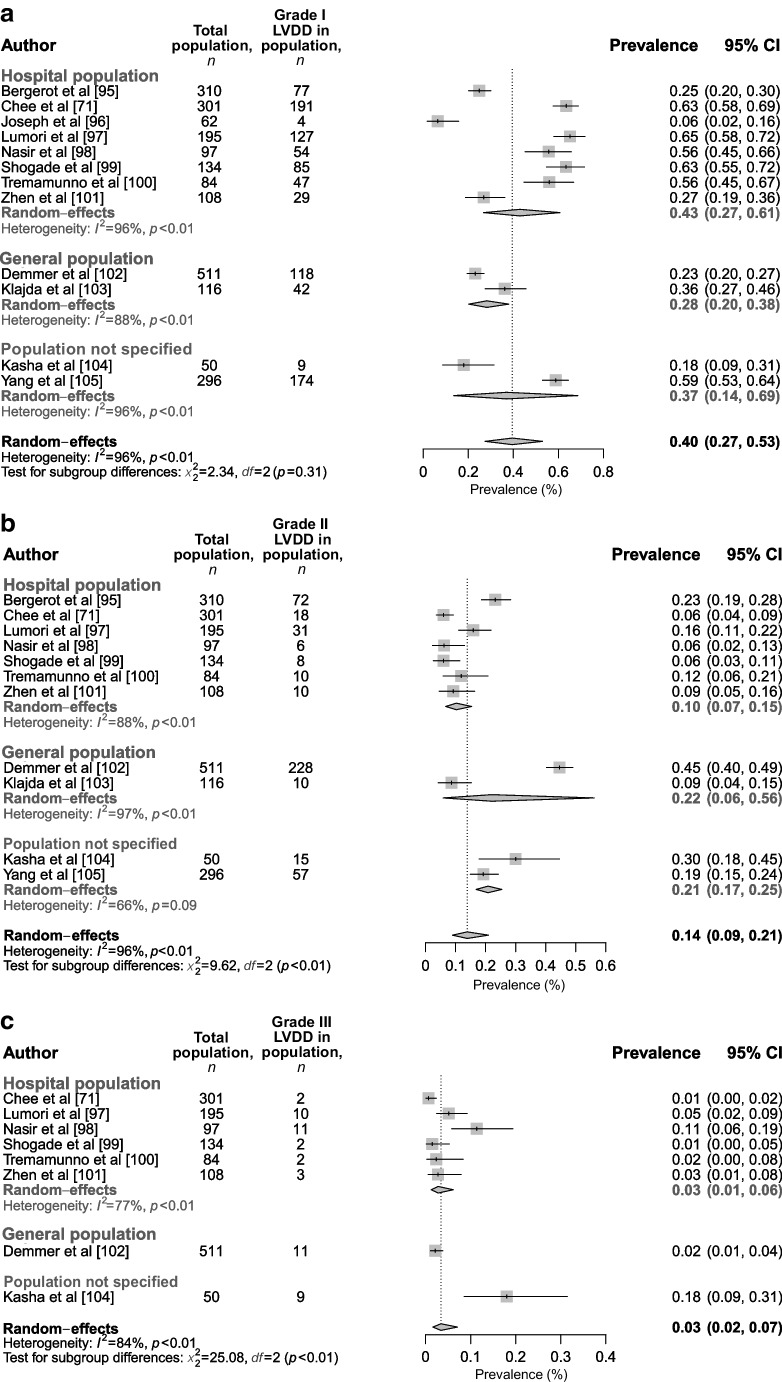
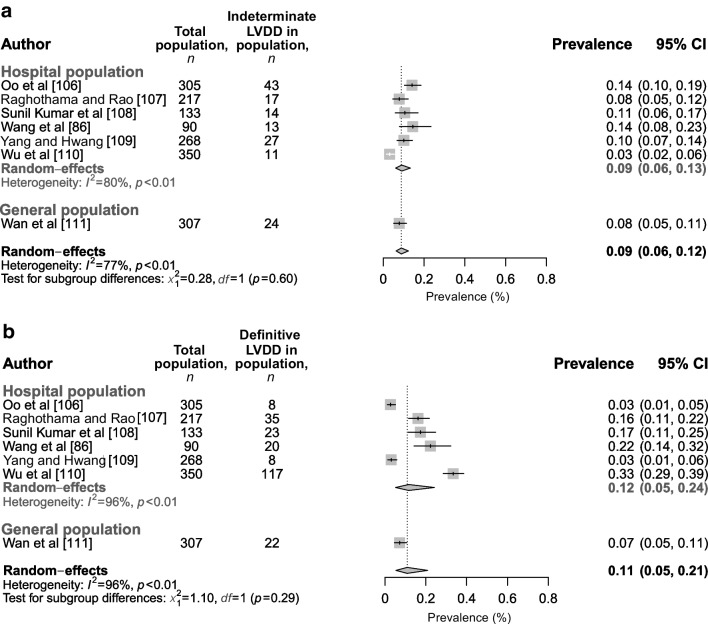
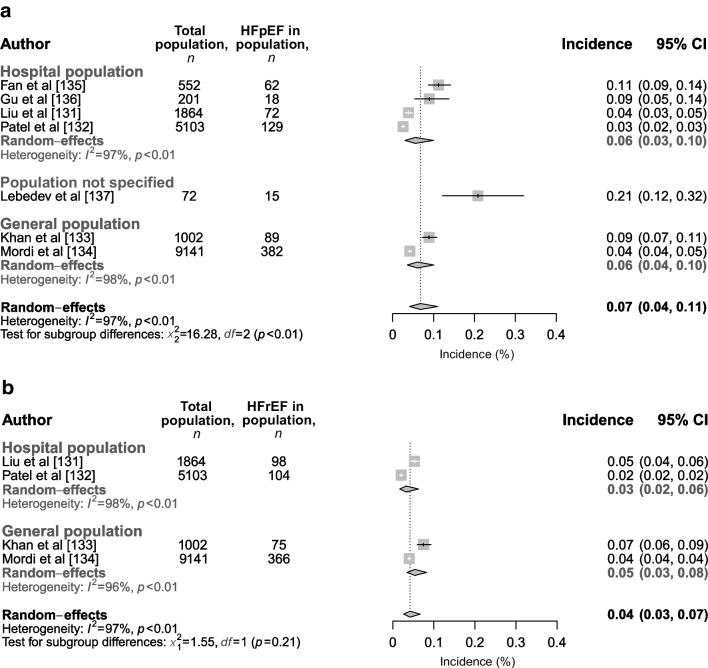
Left ventricular diastolic dysfunction (LVDD) without symptoms, and heart failure (HF) with preserved ejection fraction (HFpEF) represent the most common phenotypes of HF in individuals with type 2 diabetes mellitus, and are more common than HF with reduced ejection fraction (HFrEF), HF with mildly reduced ejection fraction (HFmrEF) and left ventricular systolic dysfunction (LVSD) in these individuals. However, diagnostic criteria for HF have changed over the years, resulting in heterogeneity in the prevalence/incidence rates reported in different studies. We aimed to give an overview of the diagnosis and epidemiology of HF in type 2 diabetes, using both a narrative and systematic review approach; we focus narratively on diagnosing (using the 2021 European Society of Cardiology [ESC] guidelines) and screening for HF in type 2 diabetes. We performed an updated (2016-October 2022) systematic review and meta-analysis of studies reporting the prevalence and incidence of HF subtypes in adults ≥18 years with type 2 diabetes, using echocardiographic data. Embase and MEDLINE databases were searched and data were assessed using random-effects meta-analyses, with findings presented as forest plots. From the 5015 studies found, 209 were screened using the full-text article. In total, 57 studies were included, together with 29 studies that were identified in a prior meta-analysis; these studies reported on the prevalence of LVSD (n=25 studies, 24,460 individuals), LVDD (n=65 studies, 25,729 individuals), HFrEF (n=4 studies, 4090 individuals), HFmrEF (n=2 studies, 2442 individuals) and/or HFpEF (n=8 studies, 5292 individuals), and on HF incidence (n=7 studies, 17,935 individuals). Using Hoy et al's risk-of-bias tool, we found that the studies included generally had a high risk of bias. They showed a prevalence of 43% (95% CI 37%, 50%) for LVDD, 17% (95% CI 7%, 35%) for HFpEF, 6% (95% CI 3%, 10%) for LVSD, 7% (95% CI 3%, 15%) for HFrEF, and 12% (95% CI 7%, 22%) for HFmrEF. For LVDD, grade I was found to be most prevalent. Additionally, we reported a higher incidence rate of HFpEF (7% [95% CI 4%, 11%]) than HFrEF 4% [95% CI 3%, 7%]). The evidence is limited by the heterogeneity of the diagnostic criteria over the years. The systematic section of this review provides new insights on the prevalence/incidence of HF in type 2 diabetes, unveiling a large pre-clinical target group with LVDD/HFpEF in which disease progression could be halted by early recognition and treatment.Registration PROSPERO ID CRD42022368035.
Keywords: Clinical research; Diabetes; Heart failure, diastolic; Heart failure, systolic; Lifestyle; Meta-analysis; Review; Systematic review.
© 2024. The Author(s).
Figures




References
-
- Adams KF, Jr, Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE) Am Heart J. 2005;149(2):209–16. doi: 10.1016/j.ahj.2004.08.005. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
