

Association of Early Dexmedetomidine Utilization With Clinical Outcomes After Moderate-Severe Traumatic Brain Injury: A Retrospective Cohort Study
- PMID: 38335145
- PMCID: PMC11250935
- DOI: 10.1213/ANE.0000000000006869
Association of Early Dexmedetomidine Utilization With Clinical Outcomes After Moderate-Severe Traumatic Brain Injury: A Retrospective Cohort Study
Abstract
Background: Traumatic brain injury (TBI) is an expensive and common public health problem. Management of TBI oftentimes includes sedation to facilitate mechanical ventilation (MV) for airway protection. Dexmedetomidine has emerged as a potential candidate for improved patient outcomes when used for early sedation after TBI due to its potential modulation of autonomic dysfunction. We examined early sedation patterns, as well as the association of dexmedetomidine exposure with clinical and functional outcomes among mechanically ventilated patients with moderate-severe TBI (msTBI) in the United States.
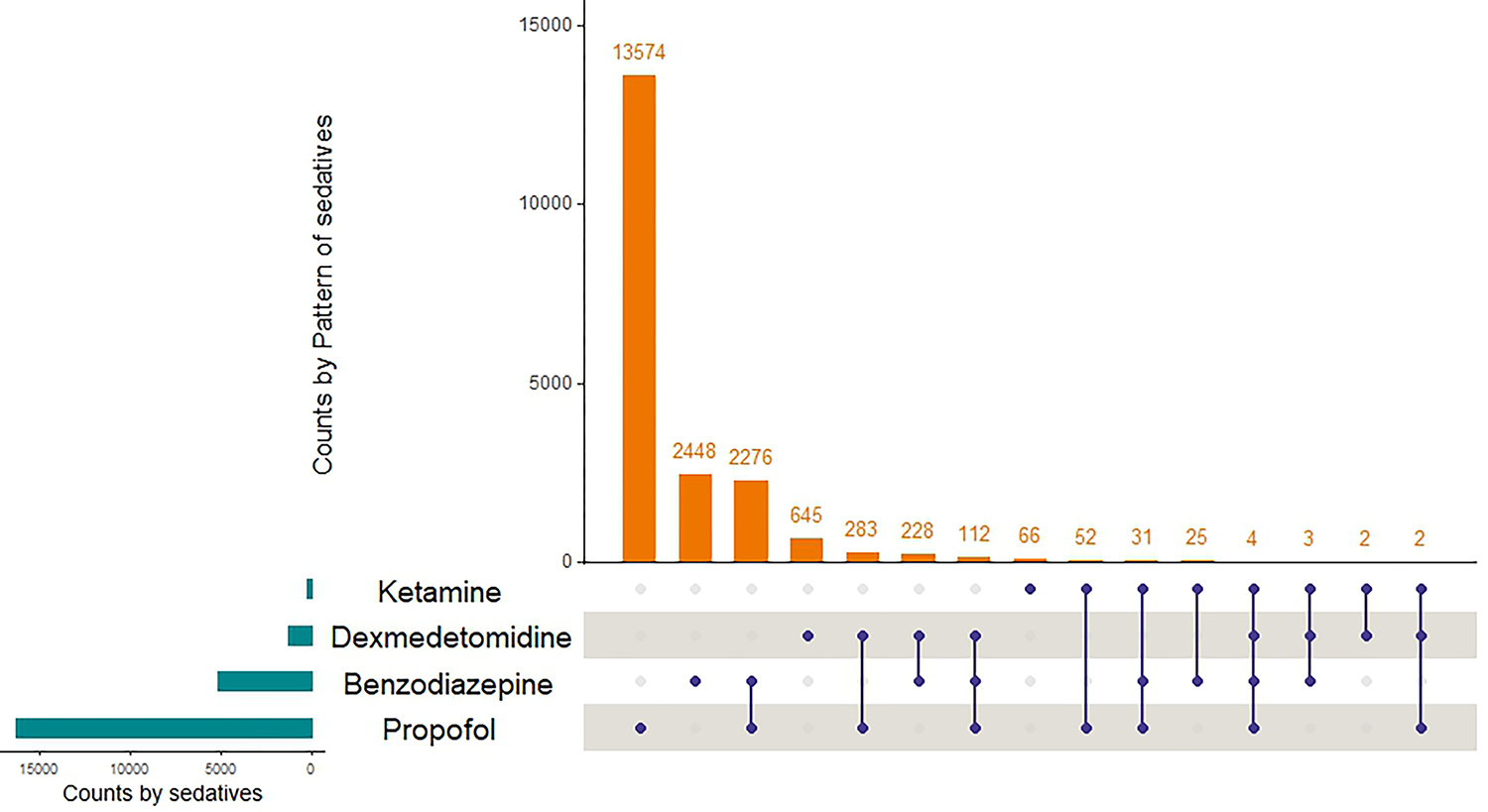
Methods: We conducted a retrospective cohort study using data from the Premier dataset and identified a cohort of critically ill adult patients with msTBI who required MV from January 2016 to June 2020. msTBI was defined by head-neck abbreviated injury scale (AIS) values of 3 (serious), 4 (severe), and 5 (critical). We described early continuous sedative utilization patterns. Using propensity-matched models, we examined the association of early dexmedetomidine exposure (within 2 days of intensive care unit [ICU] admission) with the primary outcome of hospital mortality and the following secondary outcomes: hospital length of stay (LOS), days on MV, vasopressor use after the first 2 days of admission, hemodialysis (HD) after the first 2 days of admission, hospital costs, and discharge disposition. All medications, treatments, and procedures were identified using date-stamped hospital charge codes.
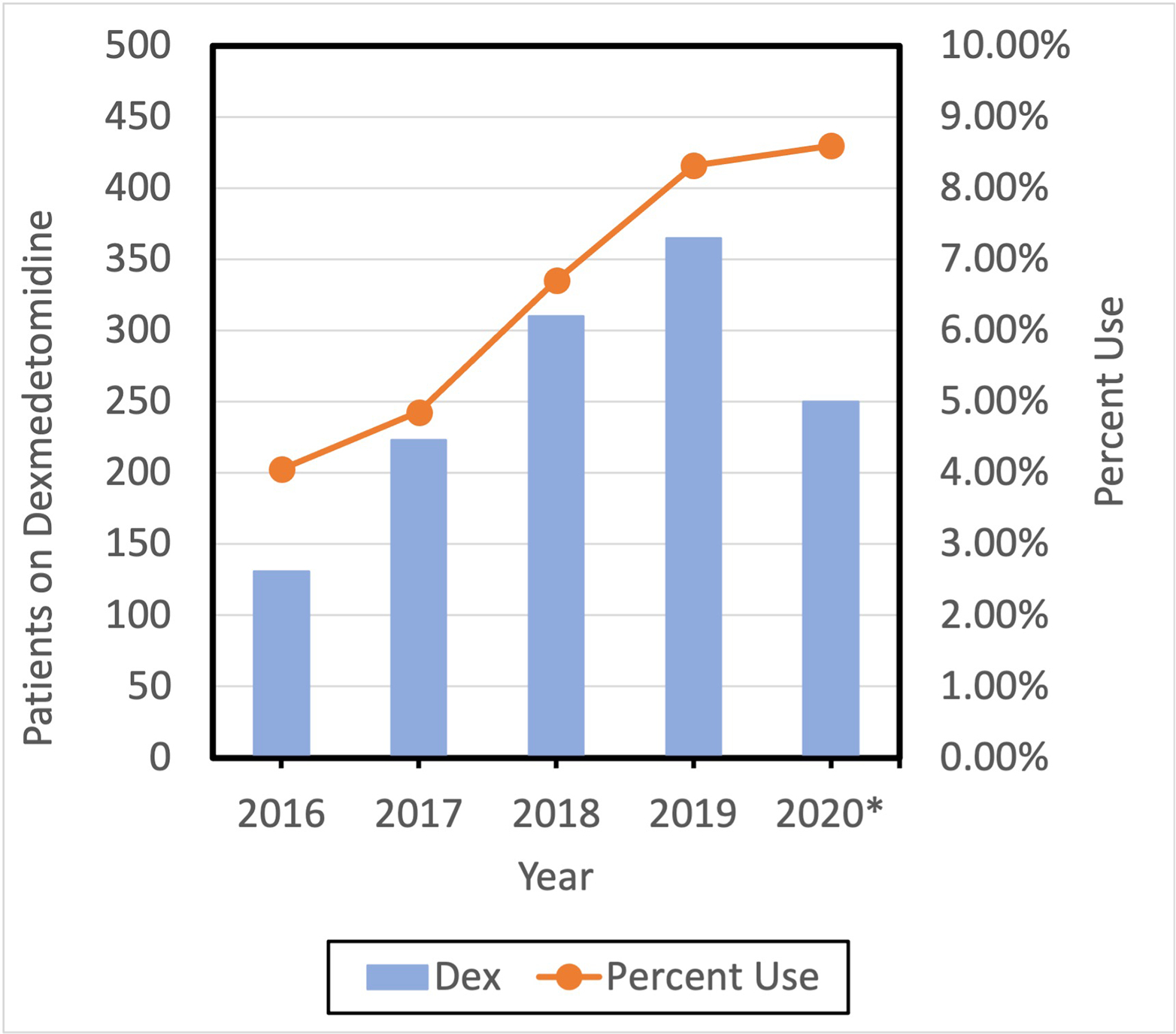
Results: The study population included 19,751 subjects who required MV within 2 days of ICU admission. The patients were majority male and white. From 2016 to 2020, the annual percent utilization of dexmedetomidine increased from 4.05% to 8.60%. After propensity score matching, early dexmedetomidine exposure was associated with reduced odds of hospital mortality (odds ratio [OR], 0.59; 95% confidence interval [CI], 0.47-0.74; P < .0001), increased risk for liberation from MV (hazard ratio [HR], 1.20; 95% CI, 1.09-1.33; P = .0003), and reduced LOS (HR, 1.11; 95% CI, 1.01-1.22; P = .033). Exposure to early dexmedetomidine was not associated with odds of HD (OR, 1.14; 95% CI, 0.73-1.78; P = .56), vasopressor utilization (OR, 1.10; 95% CI, 0.78-1.55; P = .60), or increased hospital costs (relative cost ratio, 1.98; 95% CI, 0.93-1.03; P = .66).
Conclusions: Dexmedetomidine is being utilized increasingly as a sedative for mechanically ventilated patients with msTBI. Early dexmedetomidine exposure may lead to improved patient outcomes in this population.
Copyright © 2024 International Anesthesia Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Alpha-2 agonists for sedation of mechanically ventilated adults in intensive care units: a systematic review.Health Technol Assess. 2016 Mar;20(25):v-xx, 1-117. doi: 10.3310/hta20250. Health Technol Assess. 2016. PMID: 27035758 Free PMC article.
-
Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients.Cochrane Database Syst Rev. 2015 Jan 8;1(1):CD010225. doi: 10.1002/14651858.CD010225.pub2. Cochrane Database Syst Rev. 2015. PMID: 25568981 Free PMC article.
-
Alpha-2 agonists for long-term sedation during mechanical ventilation in critically ill patients.Cochrane Database Syst Rev. 2015 Jan 6;1(1):CD010269. doi: 10.1002/14651858.CD010269.pub2. Cochrane Database Syst Rev. 2015. PMID: 25879090 Free PMC article.
-
Association between dexmedetomidine sedation and mortality in critically ill patients with ischaemic stroke: a retrospective study based on MIMIC-IV database.BMJ Open. 2025 Jul 5;15(7):e101395. doi: 10.1136/bmjopen-2025-101395. BMJ Open. 2025. PMID: 40617611 Free PMC article.
-
BIS monitoring versus clinical assessment for sedation in mechanically ventilated adults in the intensive care unit and its impact on clinical outcomes and resource utilization.Cochrane Database Syst Rev. 2018 Feb 21;2(2):CD011240. doi: 10.1002/14651858.CD011240.pub2. Cochrane Database Syst Rev. 2018. PMID: 29464690 Free PMC article.
Cited by
-
Early Intravenous Beta-Blockade with Esmolol in Adults with Severe Traumatic Brain Injury: A Phase 2a Intervention Design Study.Neurocrit Care. 2024 Dec;41(3):1009-1019. doi: 10.1007/s12028-024-02029-8. Epub 2024 Jun 28. Neurocrit Care. 2024. PMID: 38951446 Free PMC article. Clinical Trial.
-
An Overview of Adult Acute Traumatic Neurologic Injury for the Anesthesiologist: What is Known, What is New, and Emerging Concepts.Curr Anesthesiol Rep. 2025;15:22. doi: 10.1007/s40140-024-00667-4. Epub 2025 Jan 9. Curr Anesthesiol Rep. 2025. PMID: 39866534 Free PMC article.
References
-
- Krishnamoorthy V, Temkin N, Barber J, et al. Association of Early Multiple Organ Dysfunction With Clinical and Functional Outcomes Over the Year Following Traumatic Brain Injury: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury Study. Crit Care Med. Oct 1 2021;49(10):1769–1778. doi: 10.1097/CCM.0000000000005055 - DOI - PMC - PubMed
-
- Kumar RG, Kesinger MR, Juengst SB, et al. Effects of hospital-acquired pneumonia on long-term recovery and hospital resource utilization following moderate to severe traumatic brain injury. Journal of Trauma and Acute Care Surgery. 2020;88(4):491–500. doi: 10.1097/ta.0000000000002562 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
