

Risk of fractures in half a million survivors of 20 cancers: a population-based matched cohort study using linked English electronic health records
- PMID: 38335985
- PMCID: PMC10904352
- DOI: 10.1016/S2666-7568(23)00285-4
Risk of fractures in half a million survivors of 20 cancers: a population-based matched cohort study using linked English electronic health records
Abstract
Background: A history of multiple myeloma, prostate cancer, and breast cancer has been associated with adverse bone health, but associations across a broader range of cancers are unclear. We aimed to compare the risk of any bone fracture and major osteoporotic fractures in survivors of a wide range of cancers versus cancer-free individuals.
Methods: In this population-based matched cohort study, we used electronic health records from the UK Clinical Practice Research Datalink linked to hospital data. We included adults (aged ≥18 years) eligible for linkage, and we restricted the study start to Jan 2, 1998, onwards and applied administrative censoring on Jan 31, 2020. The cancer survivor group included survivors of the 20 most common cancers. Each individual with cancer was matched (age, sex, and general practice) to up to five controls (1:5) who were cancer-free. The primary outcomes were any bone fracture and any major osteoporotic fracture (pelvic, hip, wrist, spine, or proximal humeral fractures) occurring more than 1 year after index date (ie, the diagnosis date of the matched individual with cancer). We used Cox regression models, adjusted for shared risk factors, to estimate associations between cancer survivorship and bone fractures.
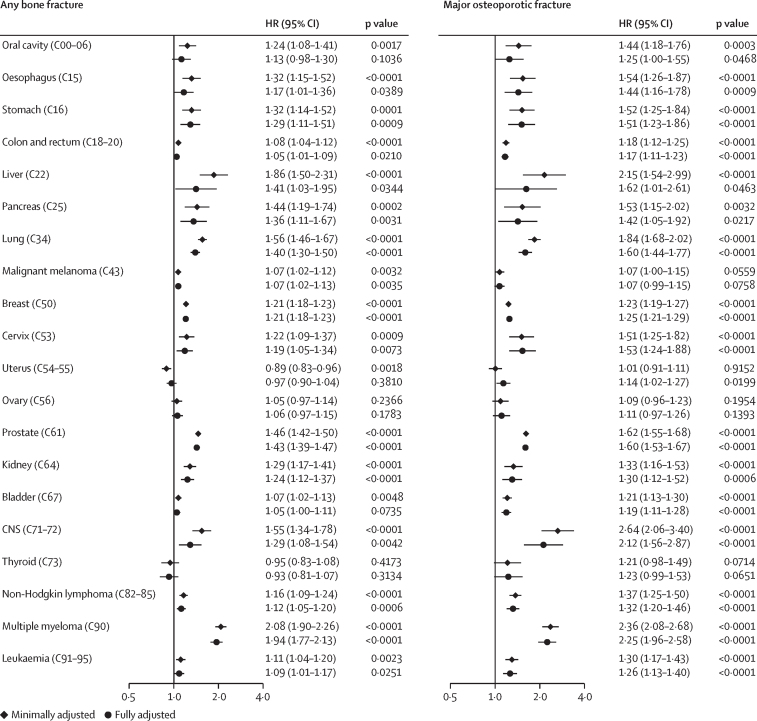
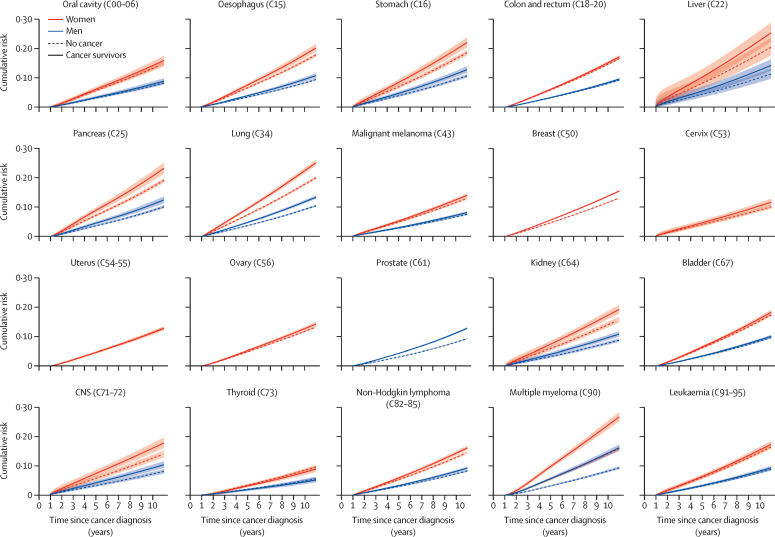
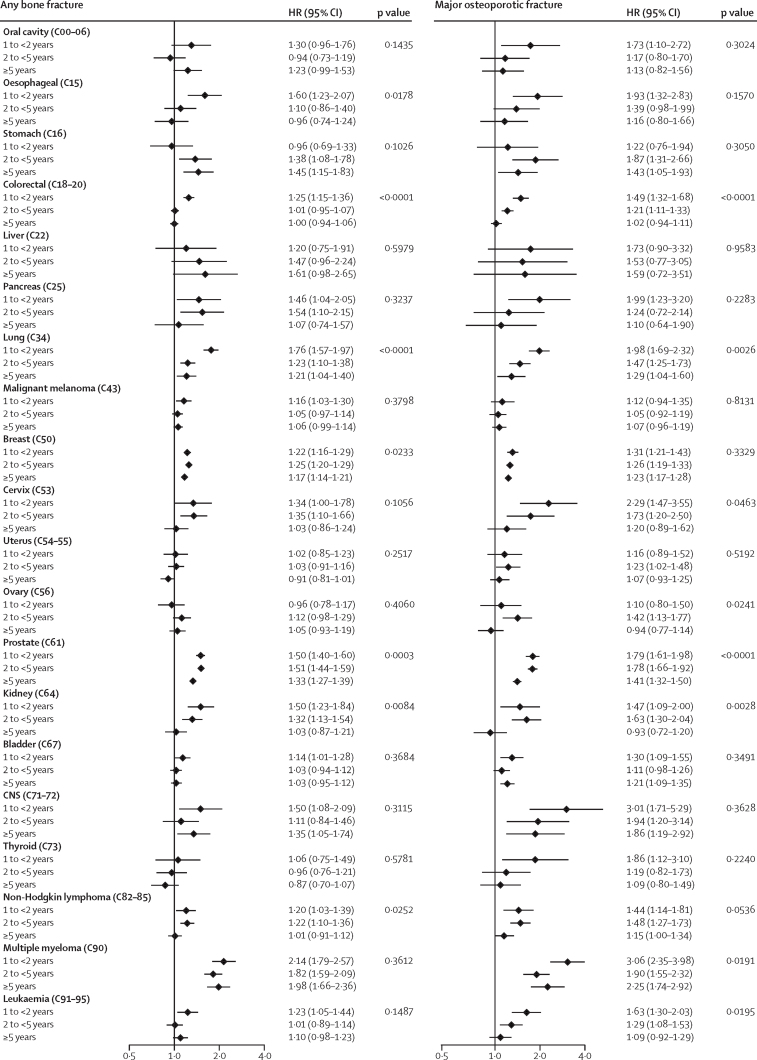
Findings: 578 160 adults with cancer diagnosed in 1998-2020 were matched to 3 226 404 cancer-free individuals. Crude incidence rates of fractures in cancer survivors ranged between 8·39 cases (95% CI 7·45-9·46) per 1000 person-years for thyroid cancer and 21·62 cases (20·18-23·18) per 1000 person-years for multiple myeloma. Compared with cancer-free individuals, the risk of any bone fracture was increased in 15 of 20 cancers, and of major osteoporotic fractures in 17 of 20 cancers. Effect sizes varied: adjusted hazard ratios (HRs) were largest for multiple myeloma (1·94, 95% CI 1·77-2·13) and prostate cancer (1·43, 1·39-1·47); HRs in the range 1·20-1·50 were seen for stomach, liver, pancreas, lung, breast, kidney, and CNS cancers; smaller associations (HR <1·20) were observed for malignant melanoma, non-Hodgkin lymphoma, leukaemia, and oesophageal, colorectal, and cervical cancers. Increased risks of major osteoporotic fracture were noted most substantially in multiple myeloma (2·25, 1·96-2·58) and CNS (2·12, 1·56-2·87), liver (1·62, 1·01-2·61), prostate (1·60, 1·53-1·67), and lung cancers (1·60, 1·44-1·77). Effect sizes tended to reduce over time since diagnosis but remained elevated for more than 5 years in several cancers, such as multiple myeloma and stomach, lung, breast, prostate, and CNS cancers.
Interpretation: Survivors of most types of cancer were at increased risk of bone fracture for several years after cancer, with variation by cancer type. These findings can help to inform mitigation and prevention strategies.
Funding: Wellcome Trust.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Cancer Research UK Cancer statistics for the UK. https://www.cancerresearchuk.org/health-professional/cancer-statistics-f...
-
- Rachner TD, Coleman R, Hadji P, Hofbauer LC. Bone health during endocrine therapy for cancer. Lancet Diabetes Endocrinol. 2018;6:901–910. - PubMed
-
- Baji P, Patel R, Judge A, et al. Organisational factors associated with hospital costs and patient mortality in the 365 days following hip fracture in England and Wales (REDUCE): a record-linkage cohort study. Lancet Healthy Longev. 2023;4:e386–e398. - PubMed
-
- Borset M, Sundan A, Waage A, Standal T. Why do myeloma patients have bone disease? A historical perspective. Blood Rev. 2020;41 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
