

Bilateral effect of acupuncture on cerebrum and cerebellum in ischaemic stroke patients with hemiparesis: a randomised clinical and neuroimaging trial
- PMID: 38336368
- PMCID: PMC11221322
- DOI: 10.1136/svn-2023-002785
Bilateral effect of acupuncture on cerebrum and cerebellum in ischaemic stroke patients with hemiparesis: a randomised clinical and neuroimaging trial
Abstract
Background: Acupuncture involving the limb region may be effective for stroke rehabilitation clinically, but the visualised and explanatory evidence is limited. Our objectives were to assess the specific effects of acupuncture for ischaemic stroke (IS) patients with hemiparesis and investigate its therapy-driven modification in functional connectivity.
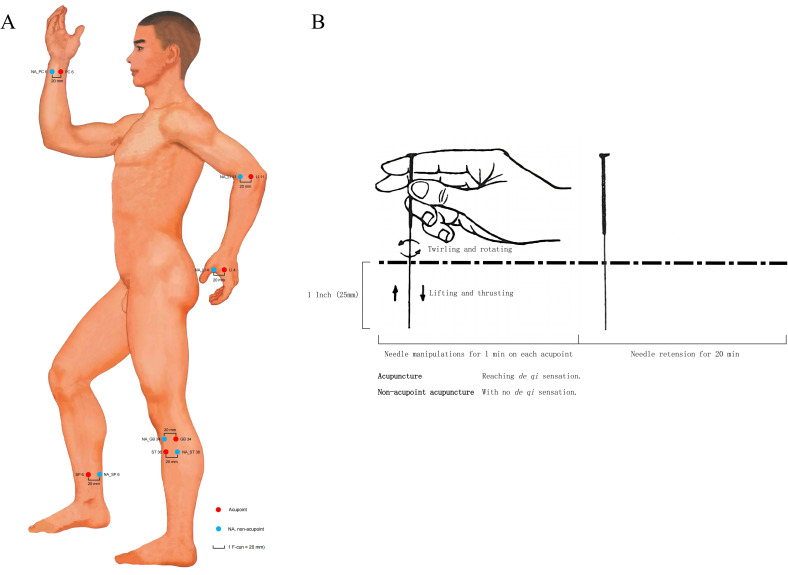
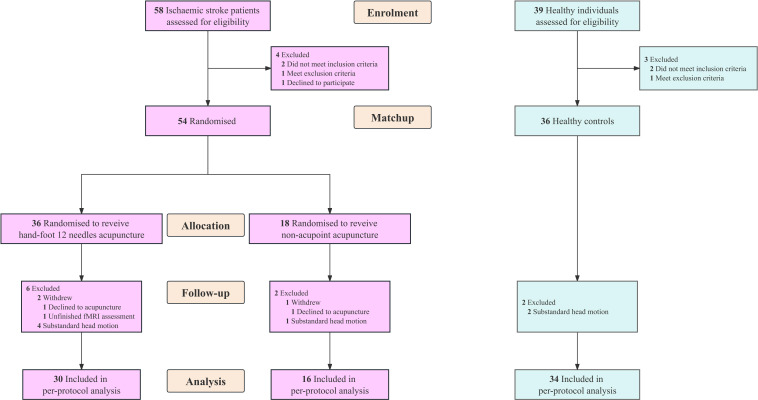
Methods: IS patients were randomly assigned (2:1) to receive 10 sessions of hand-foot 12 needles acupuncture (HA, n=30) or non-acupoint (NA) acupuncture (n=16), enrolling gender-matched and age-matched healthy controls (HCs, n=34). The clinical outcomes were the improved Fugl-Meyer Assessment scores including upper and lower extremity (ΔFM, ΔFM-UE, ΔFM-LE). The neuroimaging outcome was voxel-mirrored homotopic connectivity (VMHC). Static and dynamic functional connectivity (sFC, DFC) analyses were used to study the neuroplasticity reorganisation.
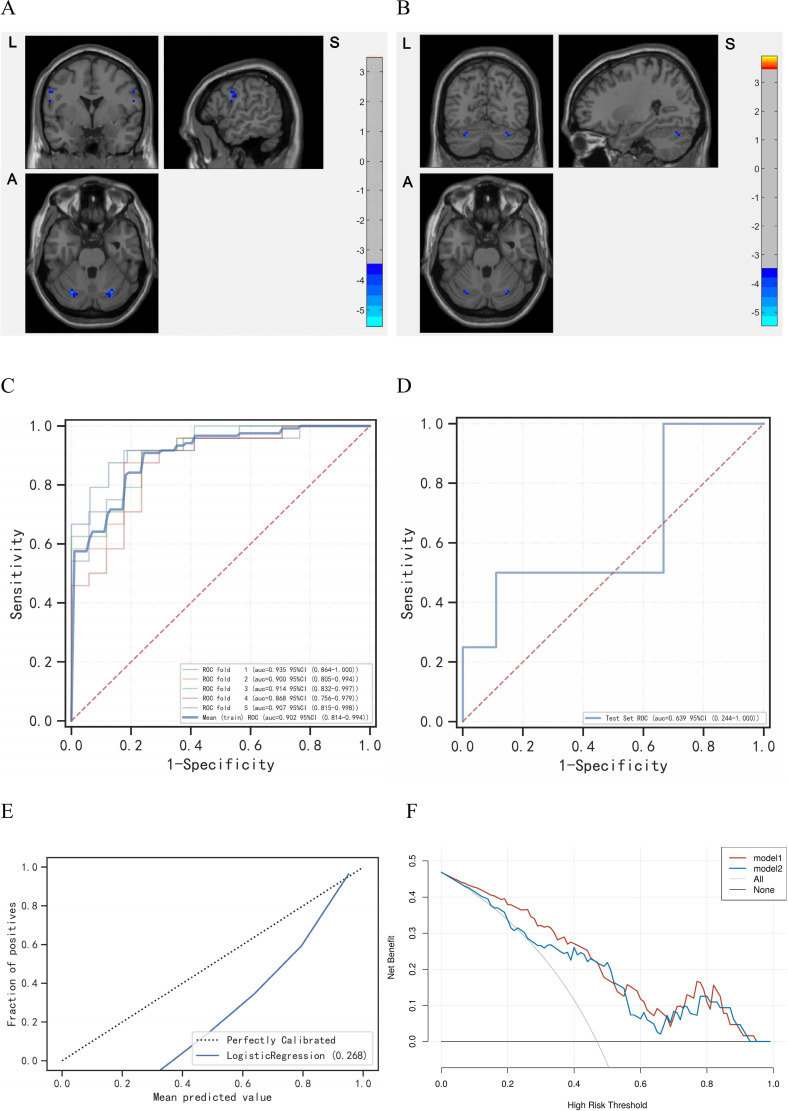
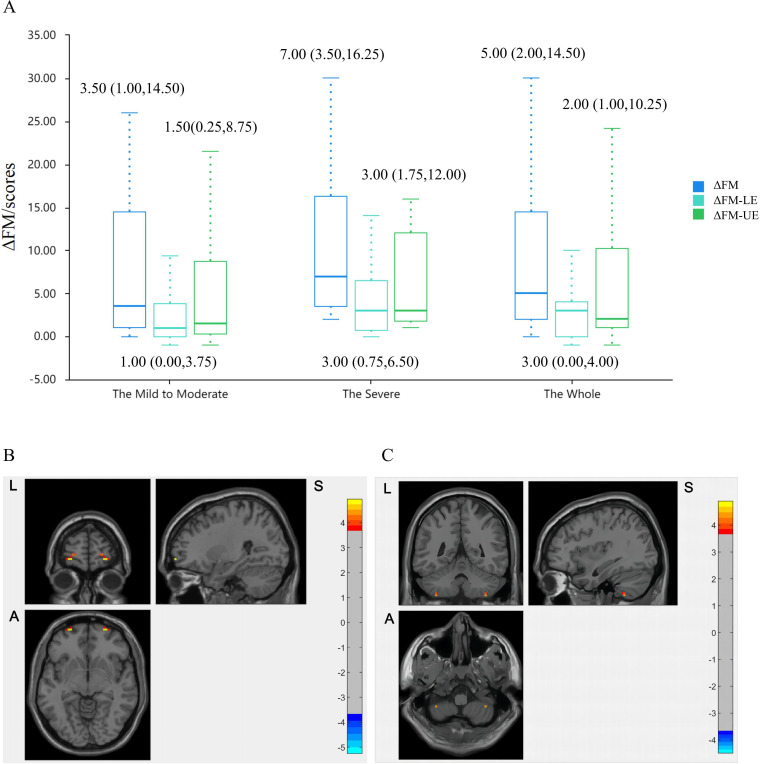
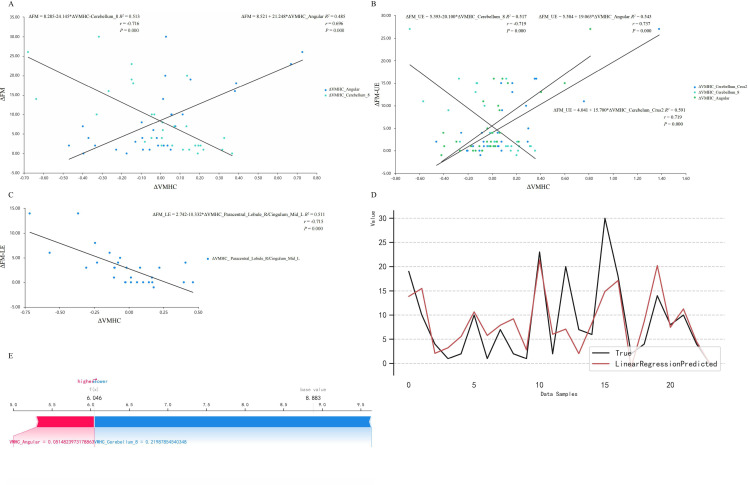
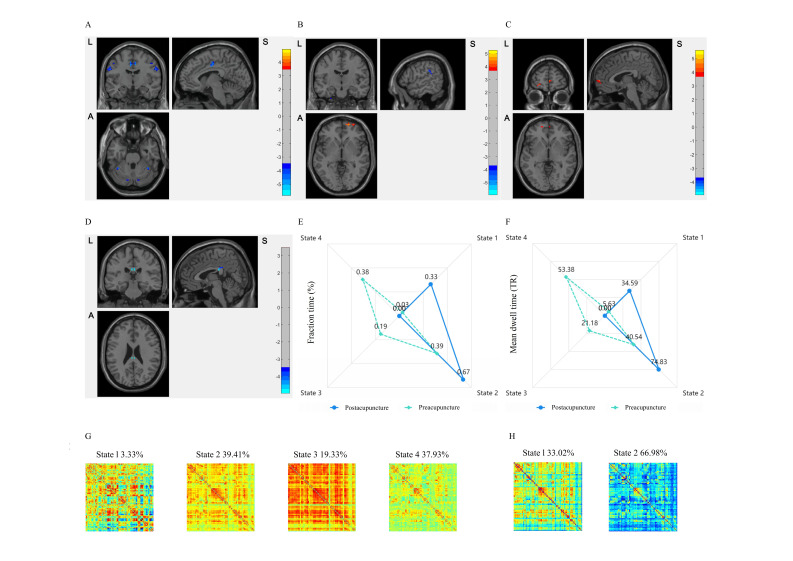
Results: 46 ISs (mean(SD) age, 59.37 (11.36) years) and 34 HCs (mean(SD) age, 52.88 (9.69) years) were included in the per-protocol analysis of clinical and neuroimaging. In clinical, ΔFM scores were 5.00 in HA group and 2.50 in NA group, with a dual correlation between ΔFM and ΔVMHC (angular: r=0.696, p=0.000; cerebellum: r=-0.716, p=0.000) fitting the linear regression model (R2=0.828). In neuroimaging, ISs demonstrated decreased VMHC in bilateral postcentral gyrus and cerebellum (Gaussian random field, GRF corrected, voxel p<0.001, cluster p<0.05), which fitted the logistic regression model (AUC=0.8413, accuracy=0.7500). Following acupuncture, VMHC in bilateral superior frontal gyrus orbital part was increased with cerebro-cerebellar changes, involving higher sFC between ipsilesional superior frontal gyrus orbital part and the contralesional orbitofrontal cortex as well as cerebellum (GRF corrected, voxel p<0.001, cluster p<0.05). The coefficient of variation of VMHC was decreased in bilateral posterior cingulate gyrus (PPC) locally (GRF corrected, voxel p<0.001, cluster p<0.05), with integration states transforming into segregation states overall (p<0.05). There was no acupuncture-related adverse event.
Conclusions: The randomised clinical and neuroimaging trial demonstrated acupuncture could promote the motor recovery and modified cerebro-cerebellar VMHC via bilateral static and dynamic reorganisations for IS patients with hemiparesis.
Keywords: Cerebral Infarction; Clinical Trial; Magnetic Resonance Imaging; Stroke; Stroke Rehabilitation.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Scalp acupuncture enhances local brain regions functional activities and functional connections between cerebral hemispheres in acute ischemic stroke patients.Anat Rec (Hoboken). 2021 Nov;304(11):2538-2551. doi: 10.1002/ar.24746. Epub 2021 Aug 25. Anat Rec (Hoboken). 2021. PMID: 34431612 Free PMC article. Clinical Trial.
-
Decreased Functional Connectivity of Homotopic Brain Regions in Chronic Stroke Patients: A Resting State fMRI Study.PLoS One. 2016 Apr 13;11(4):e0152875. doi: 10.1371/journal.pone.0152875. eCollection 2016. PLoS One. 2016. PMID: 27074031 Free PMC article.
-
Acupuncture for poststroke hemiplegia focusing on cerebral bilateral connections: study protocol for a randomised controlled neuroimaging trial.BMJ Open. 2020 Apr 1;10(4):e034548. doi: 10.1136/bmjopen-2019-034548. BMJ Open. 2020. PMID: 32241789 Free PMC article.
-
Neuroimaging of motor recovery after ischemic stroke - functional reorganization of motor network.Neuroimage Clin. 2024;43:103636. doi: 10.1016/j.nicl.2024.103636. Epub 2024 Jun 28. Neuroimage Clin. 2024. PMID: 38950504 Free PMC article. Review.
-
Advanced rehabilitation in ischaemic stroke research.Stroke Vasc Neurol. 2024 Aug 27;9(4):328-343. doi: 10.1136/svn-2022-002285. Stroke Vasc Neurol. 2024. PMID: 37788912 Free PMC article. Review.
Cited by
-
Electroacupuncture Pretreatment Reduces Ischemic Brain Injury by Inhibiting the Lactate Production and Its Derived Protein Lactylation Formation.CNS Neurosci Ther. 2025 Jan;31(1):e70231. doi: 10.1111/cns.70231. CNS Neurosci Ther. 2025. PMID: 39834103 Free PMC article.
-
Overview of evidence-based research on acupuncture for stroke treatment using magnetic resonance imaging technology.Front Neurosci. 2024 Nov 25;18:1495435. doi: 10.3389/fnins.2024.1495435. eCollection 2024. Front Neurosci. 2024. PMID: 39654647 Free PMC article. Review.
-
Neural effects of acupuncture on stroke patients with motor dysfunction: an activation likelihood estimation meta-analysis.Front Neurol. 2024 Sep 25;15:1453935. doi: 10.3389/fneur.2024.1453935. eCollection 2024. Front Neurol. 2024. PMID: 39385820 Free PMC article.
-
A bibliometric analysis of acupuncture for cerebral infarction from 1993 to 2023.Front Neurol. 2024 May 2;15:1386164. doi: 10.3389/fneur.2024.1386164. eCollection 2024. Front Neurol. 2024. PMID: 38756219 Free PMC article.
References
-
- NIH consensus conference. Acupuncture. JAMA 1998;280:1518–24. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical