

Multiomic molecular characterization of the response to combination immunotherapy in MSS/pMMR metastatic colorectal cancer
- PMID: 38336371
- PMCID: PMC10860060
- DOI: 10.1136/jitc-2023-008210
Multiomic molecular characterization of the response to combination immunotherapy in MSS/pMMR metastatic colorectal cancer
Abstract
Background: Immune checkpoint inhibitor (ICI) combinations represent an emerging treatment strategies in cancer. However, their efficacy in microsatellite stable (MSS) or mismatch repair-proficient (pMMR) colorectal cancer (CRC) is variable. Here, a multiomic characterization was performed to identify predictive biomarkers associated with patient response to ICI combinations in MSS/pMMR CRC for the further development of ICI combinations.
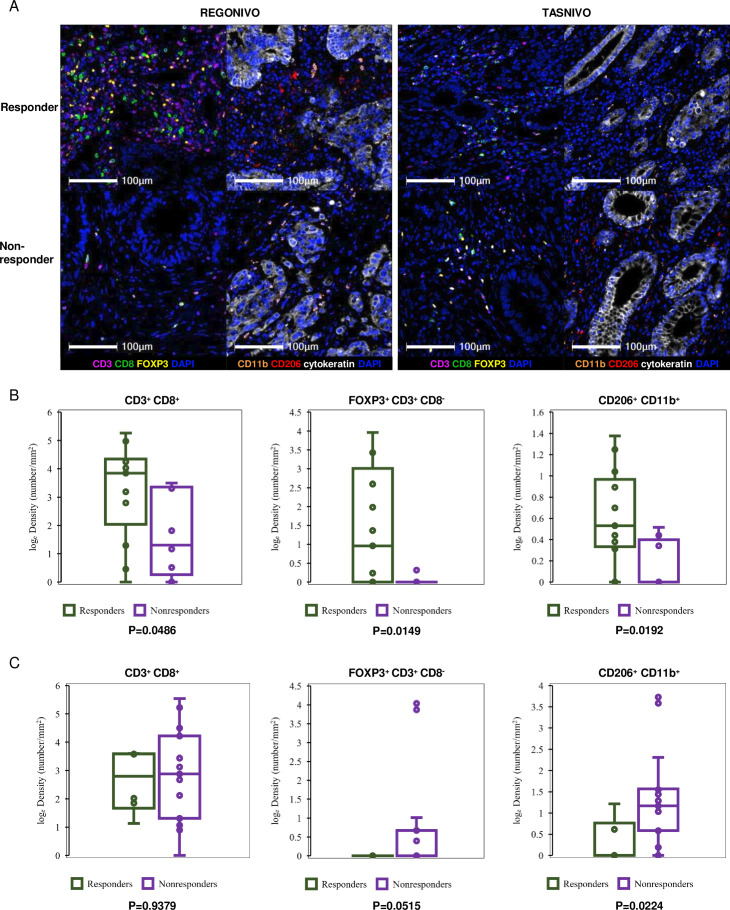
Methods: Whole-exome sequencing, RNA sequencing, and multiplex fluorescence immunohistochemistry of tumors from patients with MSS/pMMR CRC, who received regorafenib plus nivolumab (REGONIVO) or TAS-116 plus nivolumab (TASNIVO) in clinical trials were conducted. Twenty-two and 23 patients without prior ICI from the REGONIVO and TASNIVO trials were included in this study. A biomarker analysis was performed using samples from each of these studies.
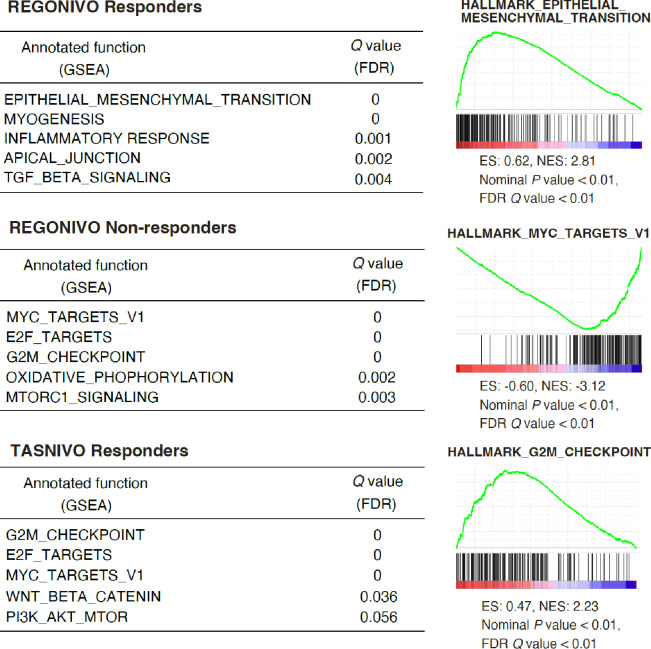
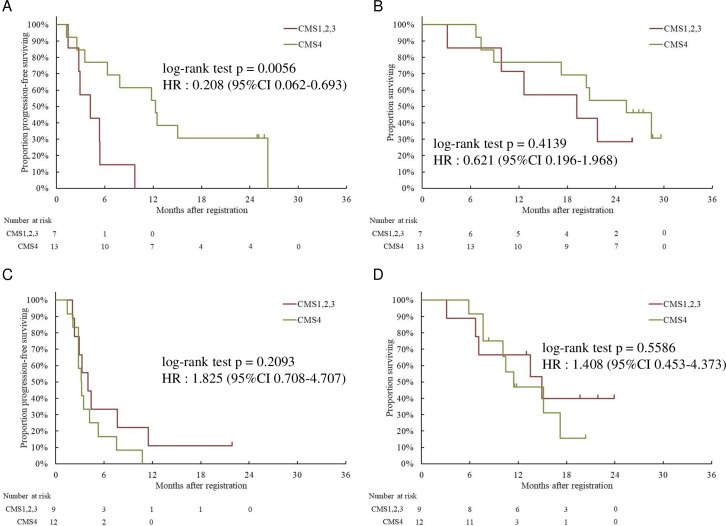
Results: The epithelial-mesenchymal transition pathway and genes related to cancer-associated fibroblasts were upregulated in the REGONIVO responder group, and the G2M checkpoint pathway was upregulated in the TASNIVO responder group. The MYC pathway was upregulated in the REGONIVO non-responder group. Consensus molecular subtype 4 was significantly associated with response (p=0.035) and longer progression-free survival (p=0.006) in the REGONIVO trial. CD8+ T cells, regulatory T cells, and M2 macrophages density was significantly higher in the REGONIVO trial responders than in non-responders. Mutations in the POLE gene and patient response were significantly associated in the TASNIVO trial; however, the frequencies of other mutations or tumor mutational burden were not significantly different between responders and non-responders in either trial.
Conclusions: We identified molecular features associated with the response to the REGONIVO and TASNIVO, particularly those related to tumor microenvironmental factors. These findings are likely to contribute to the development of biomarkers to predict treatment efficacy for MSS/pMMR CRC and future immunotherapy combinations for treatment.
Keywords: Drug Therapy, Combination; Gastrointestinal Neoplasms; Nivolumab; Tumor Biomarkers.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ST, YT, and Y-TL have nothing to disclose. SKoy has received research funding from Otsuka Pharmaceutical, Shionogi Pharmaceutical and Chugai Pharmaceutical outside the submitted work. SF has nothing to disclose. HH has received honoraria from Bayer, Bristol-Myers Squibb, Chugai, Daiichi-Sankyo, Kyowa Hakko Kirin, Lilly, Merck Biopharma, MSD, Ono, Taiho, Takeda, and Yakult; fees for consulting or advisory roles for Bristol-Myers Squibb, Boehringer Ingelheim and Daiichi-Sankyo; and research grants from ALX Oncology, Amgen, Astellas, AstraZeneca, Bayer, BeiGene, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai, Daiichi-Sankyo, Eisai, Janssen, Merck Biopharma, MSD, Ono Pharmaceutical, and Taiho Pharmaceutical outside the submitted work. YN has received honoraria from Chugai, Merck, and Guardant Health AMEA and research grants from Taiho, Chugai, Guardant Health, Genomedia, Daiichi-Sankyo, Seagen, and Roche Diagnostics outside the submitted work. YK has nothing to disclose. DK has received personal fees for advisory roles from Takeda and Eisai; honoraria from MSD, Pfizer, Chugai, Merck biopharma, Lilly, Sysmex, Nipponkayaku, Bristol-Myers Squibb, Ono Pharmaceutical, Taiho Pharmaceutical, Takeda, Eisai, and Daiichi-Sankyo; and research funding from Ono Pharmaceutical, MSD, Novartis, Sanofi, Janssen, Pierre Fabre Medicament, Isofol Medical AB, Hutchison MediPharma Limited, and Nippon Servier outside the submitted work. TKo has received honoraria from MSD, Bristol-Myers Squibb and Ono Pharmaceutical; personal fees for advisory roles from Boehringer Ingelheim, Kyowa Kirin and Taiho Pharmaceutical; and research funding from AstraZeneca, BeiGene, MSD, Amgen, Chugai Pharmaceutical, Taiho Pharmaceutical, Shionogi Pharma, and Amgen Astellas BioPharma outside the submitted work. HB has received honoraria from Ono Pharmaceutical, Taiho Pharmaceutical, and Eli Lilly Japan and research funding from Ono Pharmaceutical outside the submitted work. SM, TU, SKoj, MW, NS, and MK have nothing to disclose. TKu has received honoraria from AstraZeneca, Astellas Pharma, Ono Pharmaceutical, Bristol-Myers Squibb Japan, Daiichi-Sankyo, and Roche Diagnostics; personal fees for consulting or advisory roles from Astellas Pharma; and research funding from Daiichi-Sankyo and Roche Diagnostics outside the submitted work. TY has received research grants from Taiho, Ono, Chugai, Amgen, MSD, Daiichi-Sankyo, Eisai, FALCO biosystems, Genomedia, Molecular Health, Nippon Boehringer Ingelheim, Pfizer, Roche Diagnostics, Sysmex, and Sanofi outside the submitted work and honoraria from Bayer, Chugai, Merck Biopharma, MSD, Ono, and Takeda. HN has received research funding and honoraria from Ono Pharmaceutical, MSD, Bristol-Myers Squibb, and Chugai Pharmaceutical and research funding from Taiho Pharmaceutical, Daiichi-Sankyo, Kyowa Kirin, Zenyaku Kogyo, Oncolys BioPharma, Debiopharma, Asahi-Kasei, Sysmex, Fujifilm, SRL, Astellas Pharmaceutical, Sumitomo Dainippon Pharma, and BD Japan outside the submitted work. HM has nothing to disclose. IE has received research grants from Taiho Pharmaceutical and Ono Pharmaceutical outside the submitted work. AK has received personal fees for advisory roles from Roche and Lilly; honoraria from Roche, Merck Biopharma, Lilly, Bristol-Myers Squibb, Ono Pharmaceutical, Taiho Pharmaceutical, and Daiichi-Sankyo; and research funding from Ono Pharmaceutical, MSD, Sanofi, AstraZeneca, and Eisai outside the submitted work.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials