

Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis
- PMID: 38337355
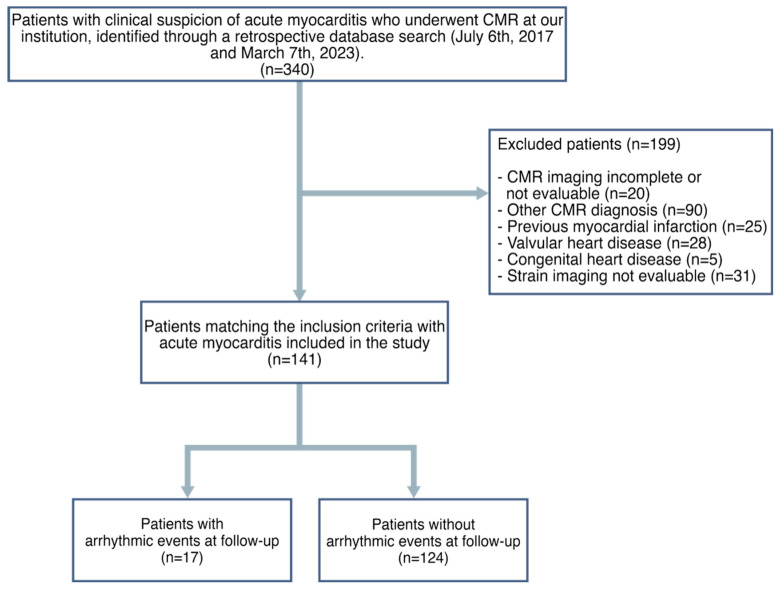
- PMCID: PMC10856157
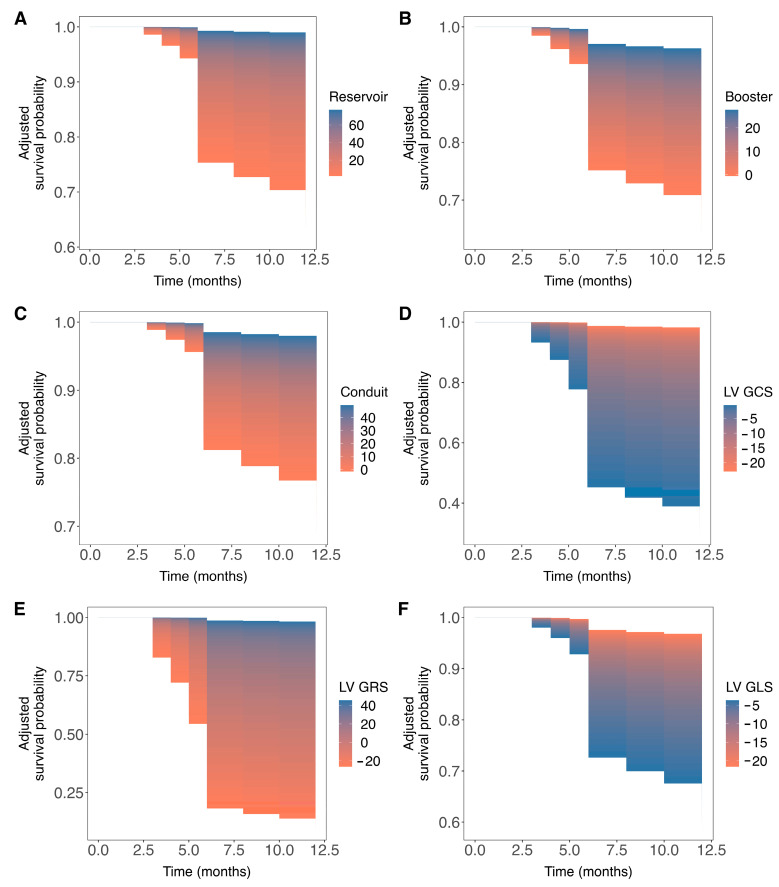
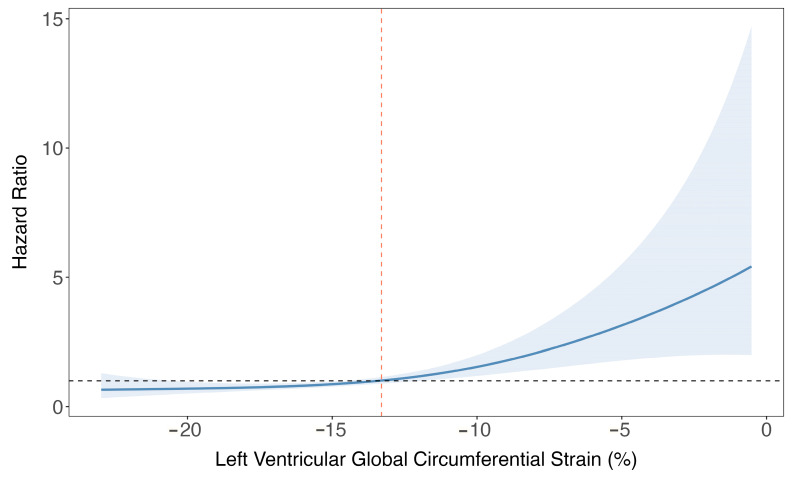
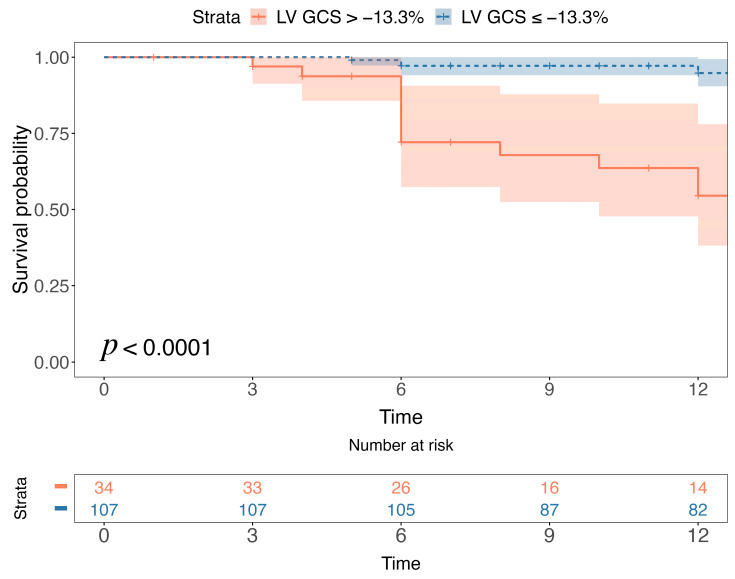
- DOI: 10.3390/jcm13030662
Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis
Abstract
(1) Objective: Myocarditis can be associated with ventricular arrhythmia (VA), individual non-invasive risk stratification through cardiovascular magnetic resonance (CMR) is of great clinical significance. Our study aimed to explore whether left atrial (LA) and left ventricle (LV) myocardial strain serve as independent predictors of VA in patients with myocarditis. (2) Methods: This retrospective study evaluated CMR scans in 141 consecutive patients diagnosed with myocarditis based on the updated Lake Louise criteria (29 females, mean age 41 ± 20). The primary endpoint was VA; this encompassed ventricular fibrillation, sustained ventricular tachycardia, nonsustained ventricular tachycardia, and frequent premature ventricular complexes. LA and LV strain function were performed on conventional cine SSFP sequences. (3) Results: After a median follow-up time of 23 months (interquartile range (18-30)), 17 patients with acute myocarditis reached the primary endpoint. In the multivariable Cox regression analysis, LA reservoir (hazard ratio [HR] and 95% confidence interval [CI]: 0.93 [0.87-0.99], p = 0.02), LA booster (0.87 95% CI [0.76-0.99], p = 0.04), LV global longitudinal (1.26 95% CI [1.02-1.55], p = 0.03), circumferential (1.37 95% CI [1.08-1.73], p = 0.008), and radial strain (0.89 95% CI [0.80-0.98], p = 0.01) were all independent determinants of VA. Patients with LV global circumferential strain > -13.3% exhibited worse event-free survival compared to those with values ≤ -13.3% (p < 0.0001). (4) Conclusions: LA and LV strain mechanism on CMR are independently associated with VA events in patients with myocarditis, independent to LV ejection fraction, and late gadolinium enhancement location. Incorporating myocardial strain parameters into the management of myocarditis may improve risk stratification.
Keywords: cardiovascular magnetic resonance; myocardial strain; myocarditis; outcomes; ventricular arrhythmia.
Conflict of interest statement
Jasjit S. Suri was employed by the company AtheroPoint™. Gianluca Pontone declares the following conflict of interest: Honorarium as speaker/consultant and/or research grant from GE Healthcare, Bracco, Heartflow, Boheringher. The remaining authors declare no conflicts of interest.
Figures
References
-
- Tschöpe C., Ammirati E., Bozkurt B., Tschöpe C., Ammirati E., Bozkurt B., Caforio A.L.P., Cooper L.T., Felix S.B., Hare J.M., et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021;18:169–193. doi: 10.1038/s41569-020-00435-x. - DOI - PMC - PubMed
-
- Ammirati E., Frigerio M., Adler E.D., Basso C., Birnie D.H., Brambatti M., Friedrich M.G., Klingel K., Lehtonen J., Moslehi J.J., et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020;13:e007405. doi: 10.1161/CIRCHEARTFAILURE.120.007405. - DOI - PMC - PubMed
-
- Ammirati E., Cipriani M., Moro C., Raineri C., Pini D., Sormani P., Mantovani R., Varrenti M., Pedrotti P., Conca C., et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients with Acute Myocarditis: Multicenter Lombardy Registry. Circulation. 2018;138:1088–1099. doi: 10.1161/CIRCULATIONAHA.118.035319. - DOI - PubMed
