

Optimal Extent of Neck Dissection for a Head and Neck Lymph Node Metastasis from a Remote Primary Site
- PMID: 38337356
- PMCID: PMC10856640
- DOI: 10.3390/jcm13030661
Optimal Extent of Neck Dissection for a Head and Neck Lymph Node Metastasis from a Remote Primary Site
Abstract
Background: Despite its rarity and limited documentation, therapeutic neck dissection (ND) for cervical lymph node (LN) metastases from distant primary sites is increasingly practiced, potentially enhancing survival rates. However, the optimal ND extent remains unclear. This study aimed to determine the safety of excluding upper neck levels from ND.
Methods: We retrospectively analyzed 25 patients who underwent ND for cervical LN metastases from remote primary tumors between 2015 and 2021 (12 with primary lung tumors, four with ovary, three with mammary gland, three with esophagus, two with thymus, and one with colon).
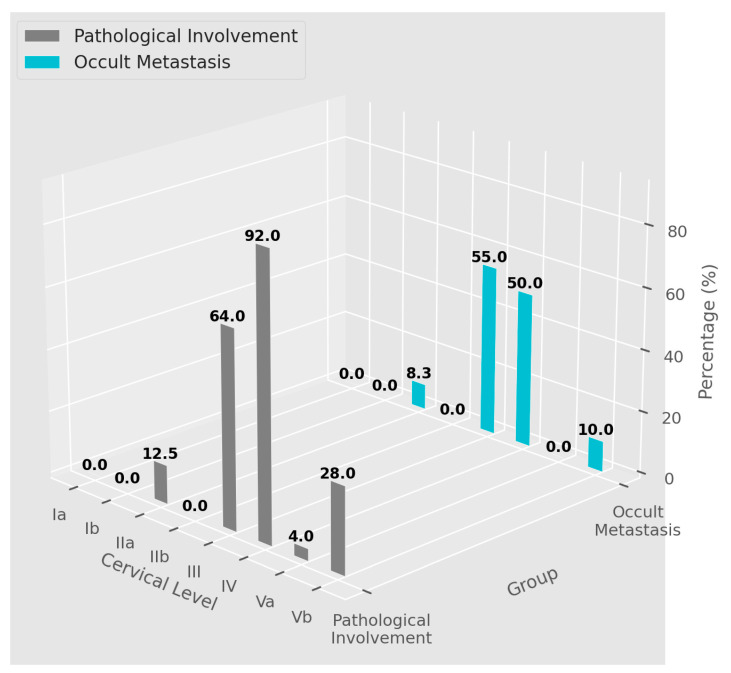
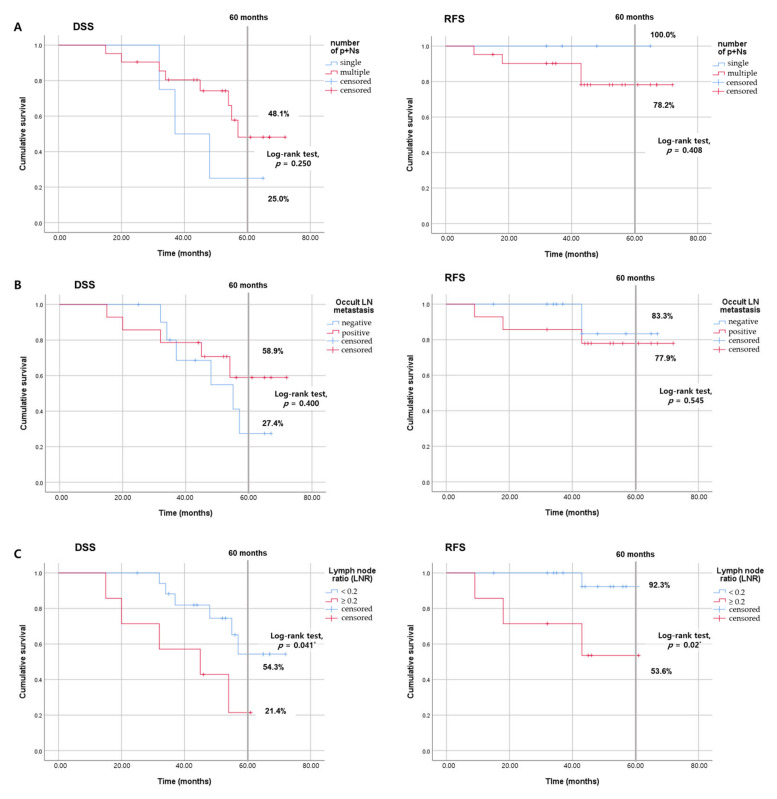
Results: Assessing clinical characteristics and occult metastasis rates, we observed LN metastases predominantly at levels III and IV. Occult metastases occurred in 14 out of 25 patients, primarily at neck levels III and IV (55.0% and 50.0%, respectively). The five-year disease-specific survival rate for all patients was 44.3%. While no statistically significant impact of occult metastasis on prognosis was confirmed, an association between the postoperative LN ratio and poor prognosis was revealed.
Conclusions: Our findings suggest that prophylactic NDs at levels I, II, and Va may not be essential for managing cervical LN metastases from remote primary malignancies. This could lead to a more tailored and less invasive therapeutic strategy.
Keywords: cervical lymph node metastasis; occult metastasis; optimal neck dissection extent; remote primary; survival.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Schiff B.A., Roberts D.B., El-Naggar A., Garden A.S., Myers J.N. Selective vs Modified Radical Neck Dissection and Postoperative Radiotherapy vs Observation in the Treatment of Squamous Cell Carcinoma of the Oral Tongue. Arch. Otolaryngol. Head Neck Surg. 2005;131:874–878. doi: 10.1001/archotol.131.10.874. - DOI - PubMed
-
- Larsen M.H., Lorenzen M.M., Bakholdt V., Sørensen J.A. The prevalence of nerve injuries following neck dissections—A systematic review and meta-analysis. Dan Med. J. 2020;67:A08190464. - PubMed
LinkOut - more resources
Full Text Sources
