

Management of Advanced Peri-Implantitis by Guided Bone Regeneration in Combination with Trabecular Metal Fixtures, Two Months after Removal of the Failed Implants: Two-Year Results of a Single-Cohort Clinical Study
- PMID: 38337407
- PMCID: PMC10856143
- DOI: 10.3390/jcm13030713
Management of Advanced Peri-Implantitis by Guided Bone Regeneration in Combination with Trabecular Metal Fixtures, Two Months after Removal of the Failed Implants: Two-Year Results of a Single-Cohort Clinical Study
Abstract
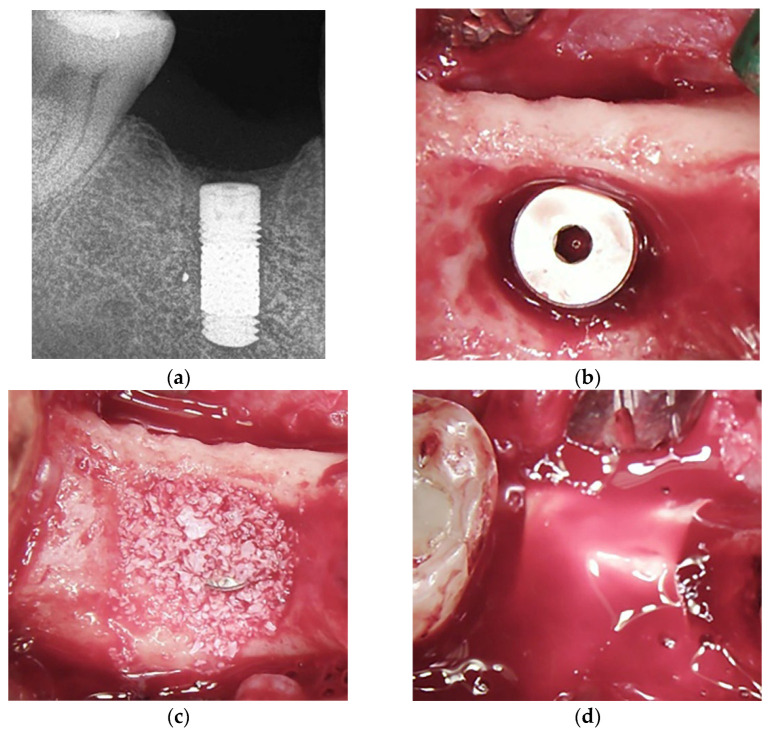
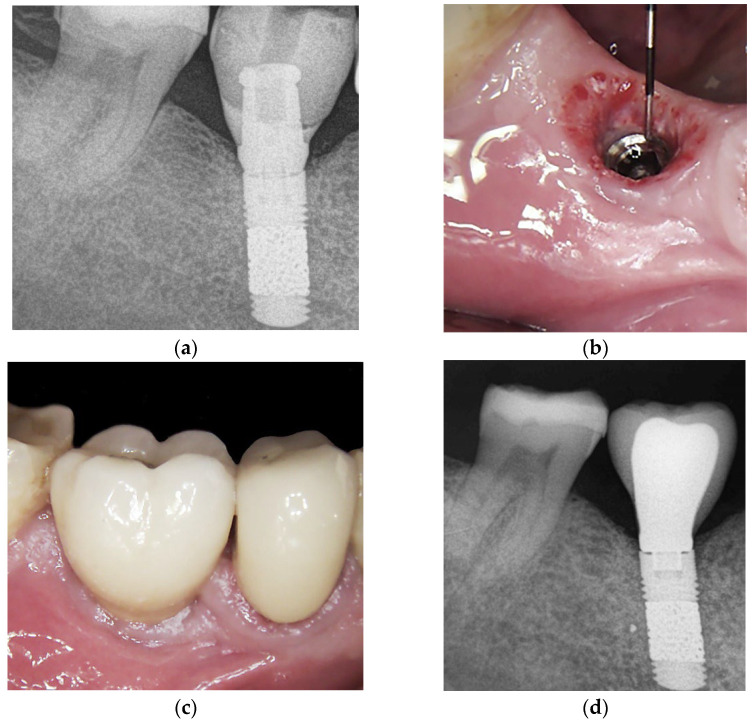
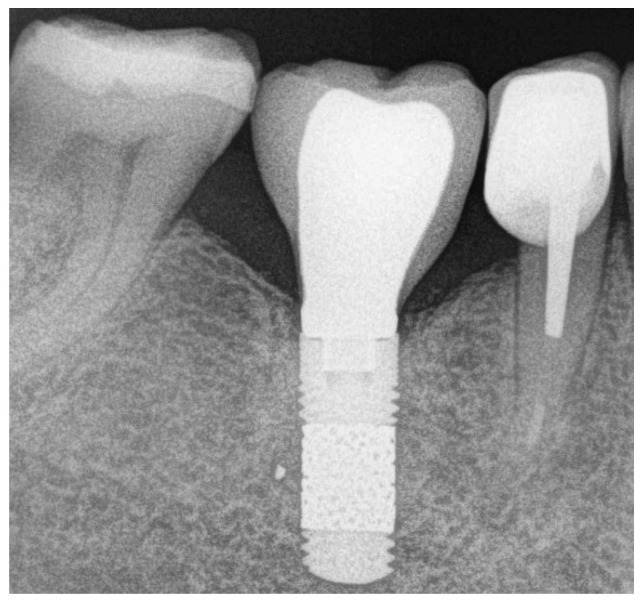
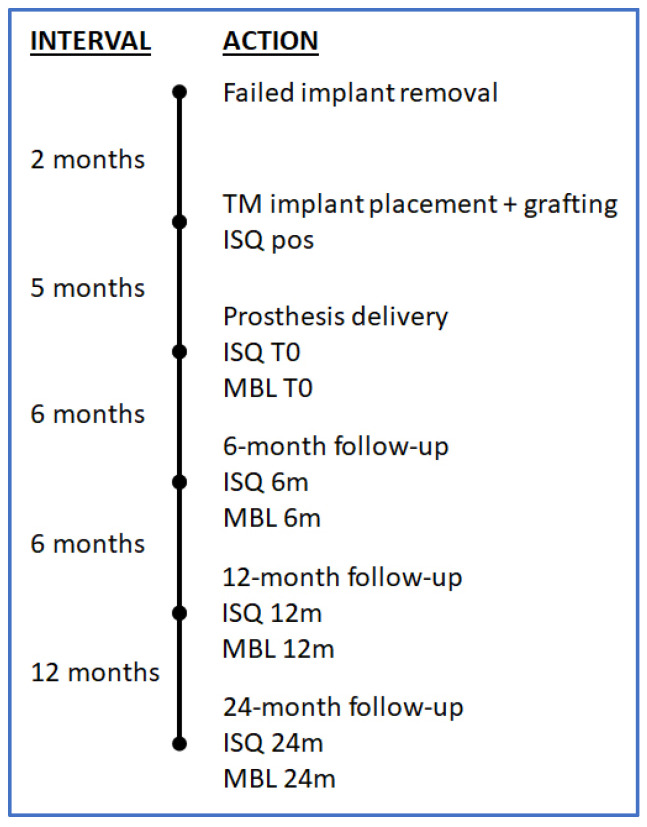
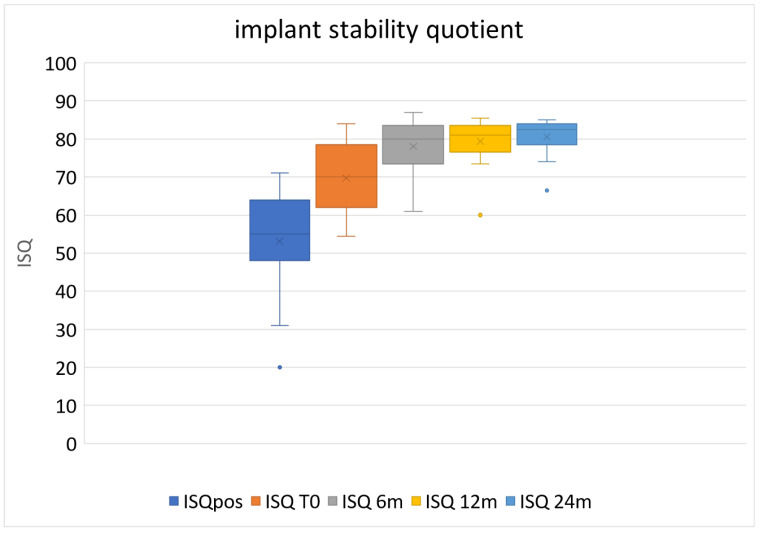
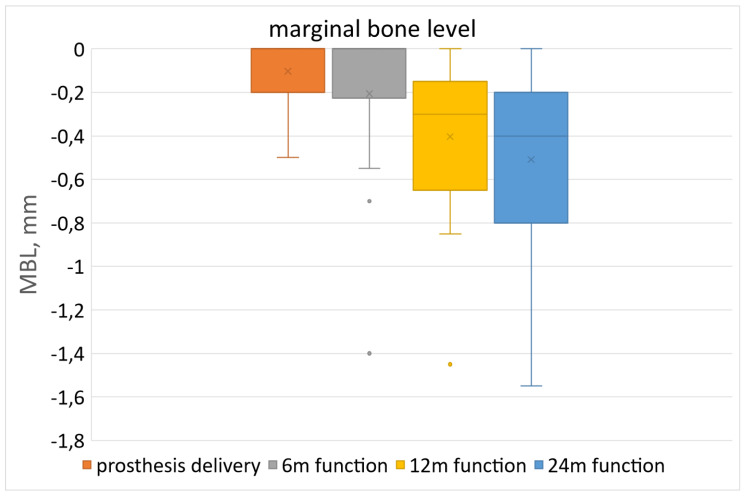
Background: Implant replacement is among the treatment options for severe peri-implantitis. The aim of this single-cohort study was to evaluate the feasibility of replacing compromised implants affected by advanced peri-implantitis with new implants with a porous trabecular metal (TM) structure. Materials and Methods: Patients with one or more implants in the posterior region showing a defect depth >50% of implant length, measured from the residual crest, were consecutively included. Two months after implant removal, patients received a TM implant combined with a xenograft and a resorbable membrane. The implant stability quotient (ISQ) was measured at placement and re-assessed five months later (at uncovering), then after 6, 12, and 24 months of function. Marginal bone loss was radiographically evaluated. Results: Twenty consecutive cases were included. One patient dropped out due to COVID-19 infection, and nineteen cases were evaluated up to 24 months. At placement, the mean ISQ was 53.08 ± 13.65 (standard deviation), which increased significantly to 69.74 ± 9.01 after five months of healing (p < 0.001) and to 78.00 ± 7.29 after six months of loading (p < 0.001). Thereafter, the ISQ remained stable for up to 24 months (80.55 ± 4.73). All implants successfully osseointegrated and were restored as planned. After two years, the average marginal bone level change was -0.41 ± 0.38 mm (95% confidence interval -0.60, -0.21), which was limited yet significantly different from the baseline (p < 0.05). Conclusions: The treatment of advanced peri-implant defects using TM implants inserted two months after explantation in combination with guided bone regeneration may achieve successful outcomes up to two years follow-up, even in the presence of low primary stability.
Keywords: dental implants; guided bone regeneration; implant explantation; implant stability; osseointegration; peri-implantitis; surgical treatment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Early postextraction implants may achieve osseointegration in the absence of primary stability. A pilot study.J Biol Regul Homeost Agents. 2019 Nov-Dec;33(6 Suppl. 2):1-12. DENTAL SUPPLEMENT. J Biol Regul Homeost Agents. 2019. PMID: 32425019
-
Long time follow up of implant therapy and treatment of peri-implantitis.Swed Dent J Suppl. 2007;(188):7-66. Swed Dent J Suppl. 2007. PMID: 17694834
-
Clinical outcomes of dental implants placed in the same region where previous implants failed due to peri-implantitis: a retrospective study.Int J Implant Dent. 2021 Nov 9;7(1):109. doi: 10.1186/s40729-021-00392-1. Int J Implant Dent. 2021. PMID: 34751830 Free PMC article.
-
Bone regeneration as treatment of peri-implant disease: A narrative review.Clin Implant Dent Relat Res. 2023 Aug;25(4):696-709. doi: 10.1111/cid.13209. Epub 2023 May 17. Clin Implant Dent Relat Res. 2023. PMID: 37199027 Review.
-
Initial and long-term crestal bone responses to modern dental implants.Periodontol 2000. 2017 Feb;73(1):41-50. doi: 10.1111/prd.12176. Periodontol 2000. 2017. PMID: 28000272 Review.
References
-
- Albrektsson T., Isidor F. Consensus report of session IV. In: Lang N.P., Karring T., editors. Proceedings of the First European Workshop on Periodontology; Warth-Weiningen, Switzerland. 1–4 February 1993; London, UK: Quintessence; 1994. pp. 365–369.
-
- Berglundh T., Armitage G., Araujo M.G., Avila-Ortiz G., Blanco J., Camargo P.M., Chen S., Cochran D., Derks J., Figuero E., et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018;45((Suppl. S20)):S286–S291. doi: 10.1111/jcpe.12957. - DOI - PubMed
-
- Schmid E., Eick S., Sculean A., Salvi G.E. Peri-Implant Diseases: Characteristics of the Microbiota and of the Host Response in Humans—A Narrative Review. Monogr. Oral Sci. 2021;29:98–104. - PubMed
