

Platelets and Thrombotic Antiphospholipid Syndrome
- PMID: 38337435
- PMCID: PMC10856779
- DOI: 10.3390/jcm13030741
Platelets and Thrombotic Antiphospholipid Syndrome
Abstract
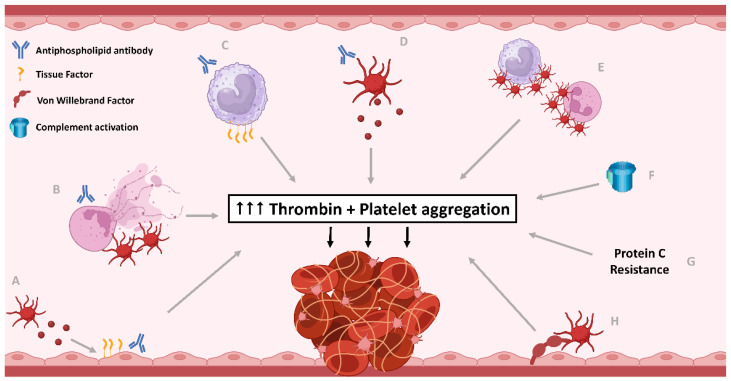
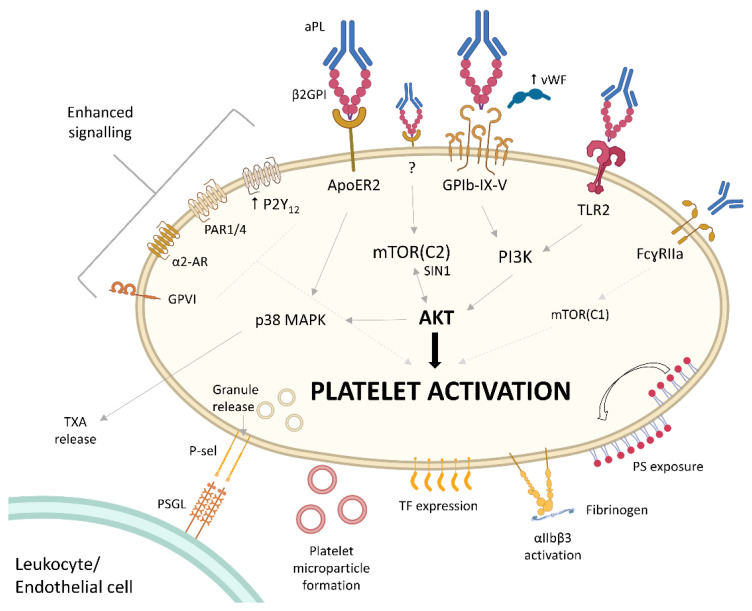
Antiphospholipid antibody syndrome (APS) is an autoimmune disorder characterised by thrombosis and the presence of antiphospholipid antibodies (aPL): lupus anticoagulant and/or IgG/IgM anti-β2-glycoprotein I and anticardiolipin antibodies. APS carries significant morbidity for a relatively young patient population from recurrent thrombosis in any vascular bed (arterial, venous, or microvascular), often despite current standard of care, which is anticoagulation with vitamin K antagonists (VKA). Platelets have established roles in thrombosis at any site, and platelet hyperreactivity is clearly demonstrated in the pathophysiology of APS. Together with excess thrombin generation, platelet activation and aggregation are the common end result of all the pathophysiological pathways leading to thrombosis in APS. However, antiplatelet therapies play little role in APS, reserved as a possible option of low dose aspirin in addition to VKA in arterial or refractory thrombosis. This review outlines the current evidence and mechanisms for excessive platelet activation in APS, how it plays a central role in APS-related thrombosis, what evidence for antiplatelets is available in clinical outcomes studies, and potential future avenues to define how to target platelet hyperreactivity better with minimal impact on haemostasis.
Keywords: antiphospholipid antibodies; antiphospholipid syndrome; antiplatelets; platelets; thrombosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Miyakis S., Lockshin M.D., Atsumi T., Branch D.W., Brey R.L., Cervera R., Derksen R.H.W.M., De Groot P.G., Koike T., Meroni P.L., et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J. Thromb. Haemost. 2006;4:295–306. doi: 10.1111/j.1538-7836.2006.01753.x. - DOI - PubMed
-
- Sevim E., Zisa D., Andrade D., Sciascia S., Pengo V., Tektonidou M.G., Ugarte A., Gerosa M., Belmont H.M., Zamorano M.A.A., et al. Characteristics of Patients with Antiphospholipid Antibody Positivity in the APS ACTION International Clinical Database and Repository. Arthritis Care Res. 2022;74:324–335. doi: 10.1002/acr.24468. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
