

Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study
- PMID: 38337497
- PMCID: PMC10856481
- DOI: 10.3390/jcm13030802
Evaluation of the Efficacy and Safety of Quetiapine in the Treatment of Delirium in Adult ICU Patients: A Retrospective Comparative Study
Abstract
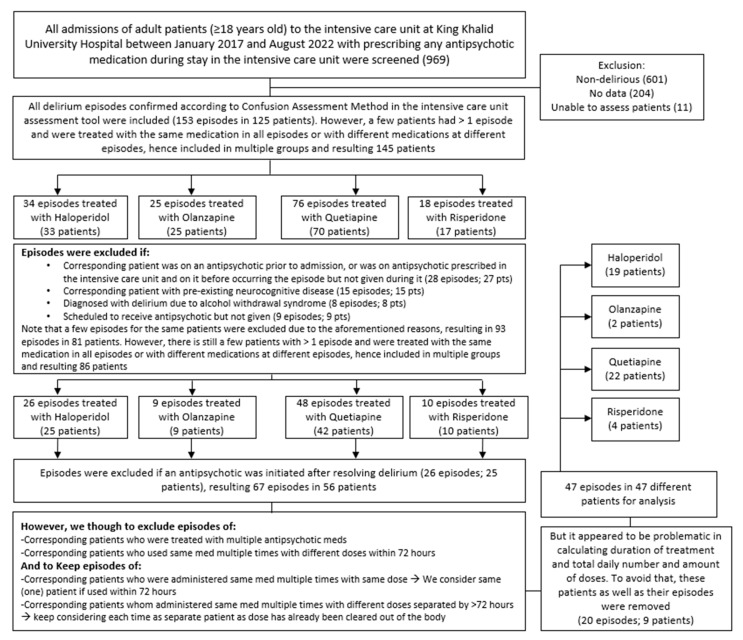
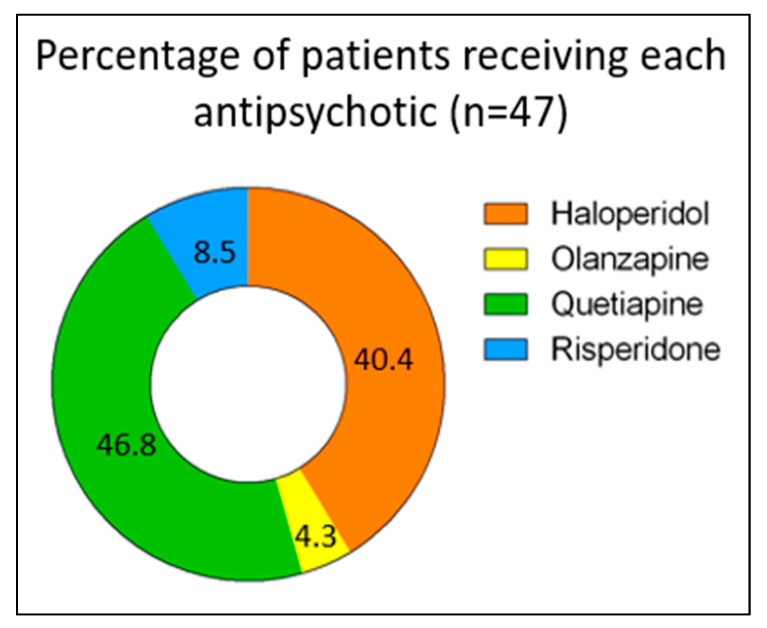
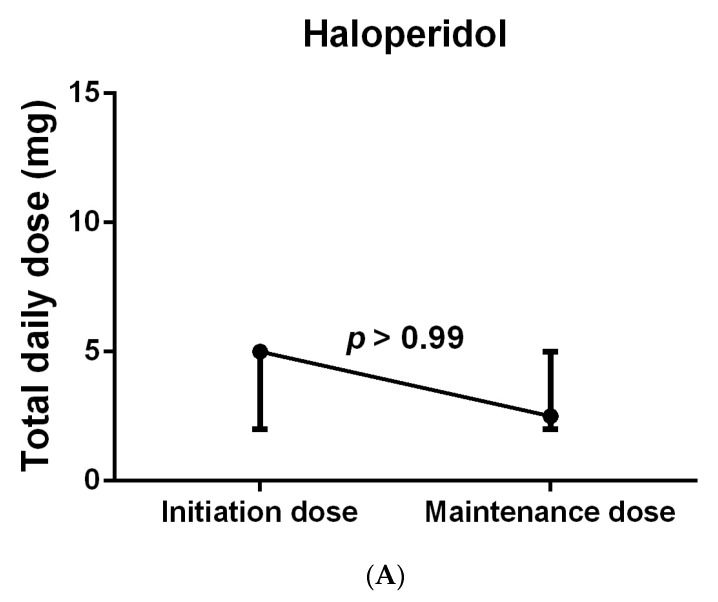
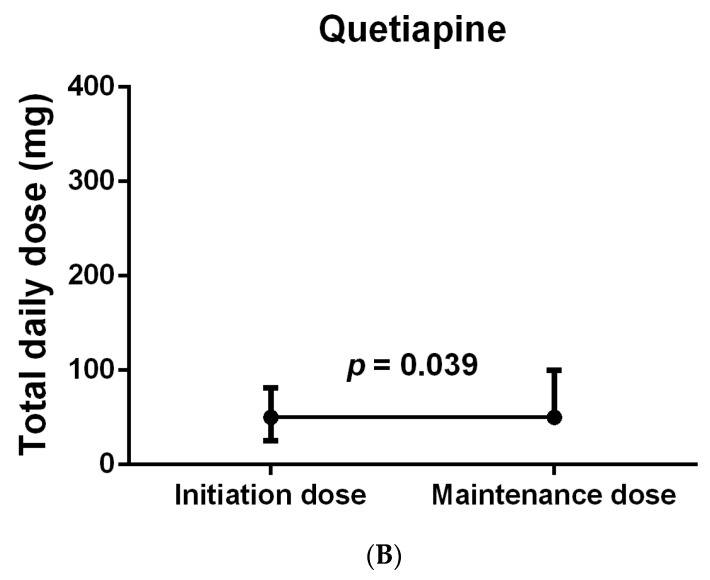
Background: Quetiapine is commonly prescribed off-label to manage delirium in intensive care unit (ICU) patients. However, limited studies comparing its efficacy and safety to those of other antipsychotics exist in the literature. Method: A retrospective, single-center chart review study was conducted on adults admitted to the ICU between January 2017 and August 2022, who were diagnosed with delirium and treated with a single antipsychotic and had no neurological medical conditions, active alcohol withdrawal, or prior use of antipsychotics. Data were analyzed using SPSS software version 28, with p-values of <0.05 indicating statistical significance. Results: In total, 47 patients were included, of whom 22 (46.8%), 19 (40.4%), 4 (8.5%), and 2 (4.3%) were on quetiapine, haloperidol, risperidone, and olanzapine, respectively. The median number of hours needed to resolve delirium were 12 (21.5), 23 (28), 13 (13.75), and 36 (10) (p = 0.115) for quetiapine, haloperidol, risperidone, and olanzapine, respectively, with haloperidol being used for a significantly shorter median number of days than quetiapine (3 (2.5) days vs. 7.5 (11.5) days; p = 0.007). Of the medication groups, only quetiapine-treated patients received a significantly higher median maintenance compared to the initiation dose (50 (50) mg vs. 50 (43.75) mg; p = 0.039). For the length of stay in the ICU and hospital, delirium-free days, % of ICU time spent in delirium, ventilator-free days, the difference between the highest and baseline QTc intervals, and ICU and hospital mortalities, no significant difference was observed between the groups. Conclusions: Overall, the use of quetiapine in our retrospective study seems to not be advantageous over the other drugs in terms of efficacy and safety outcomes.
Keywords: ICU; QTc interval; delirium; efficacy and safety; haloperidol; olanzapine; quetiapine; risperidone.
Conflict of interest statement
The authors declare they have no competing interests.
Figures
Similar articles
-
Comparison of Lurasidone Versus Quetiapine for the Treatment of Delirium in Critically Ill Patients.J Intensive Care Med. 2020 Apr;35(4):394-399. doi: 10.1177/0885066617754187. Epub 2018 Jan 22. J Intensive Care Med. 2020. PMID: 29357776
-
Quetiapine Twice Daily Versus Bedtime Dosing in the Treatment of ICU Delirium.J Pharm Pract. 2024 Aug;37(4):945-949. doi: 10.1177/08971900231193545. Epub 2023 Aug 1. J Pharm Pract. 2024. PMID: 37527549
-
Pharmacologic Management of Intensive Care Unit Delirium: Clinical Prescribing Practices and Outcomes in More Than 8500 Patient Encounters.Anesth Analg. 2021 Sep 1;133(3):713-722. doi: 10.1213/ANE.0000000000005365. Anesth Analg. 2021. PMID: 33433117 Free PMC article.
-
Antipsychotics for the prevention and treatment of delirium in the intensive care unit: what is their role?Harv Rev Psychiatry. 2011 Mar-Apr;19(2):59-67. doi: 10.3109/10673229.2011.565247. Harv Rev Psychiatry. 2011. PMID: 21425934 Review.
-
Antipsychotic Use in the Prevention and Treatment of Intensive Care Unit Delirium in Pediatric Patients.J Pediatr Pharmacol Ther. 2020;25(2):81-95. doi: 10.5863/1551-6776-25.2.81. J Pediatr Pharmacol Ther. 2020. PMID: 32071582 Free PMC article. Review.
Cited by
-
Quetiapine Use Is Associated with Longer ICU Stay Compared to Control and Haloperidol: A Propensity Score-Matched Analysis Using the MIMIC-IV Database.J Clin Med. 2025 Jun 23;14(13):4438. doi: 10.3390/jcm14134438. J Clin Med. 2025. PMID: 40648812 Free PMC article.
-
The Role of Quetiapine in Treating Delirium in Critical Care Settings: A Narrative Review.J Clin Med. 2025 Apr 18;14(8):2798. doi: 10.3390/jcm14082798. J Clin Med. 2025. PMID: 40283628 Free PMC article. Review.
References
-
- Barr J., Fraser G.L., Puntillo K., Ely E.W., Gélinas C., Dasta J.F., Davidson J.E., Devlin J.W., Kress J.P., Joffe A.M., et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit. Care Med. 2013;41:263–306. doi: 10.1097/CCM.0b013e3182783b72. - DOI - PubMed
LinkOut - more resources
Full Text Sources
