

Advances in Multi-Modality Imaging in Hypertrophic Cardiomyopathy
- PMID: 38337535
- PMCID: PMC10856479
- DOI: 10.3390/jcm13030842
Advances in Multi-Modality Imaging in Hypertrophic Cardiomyopathy
Abstract
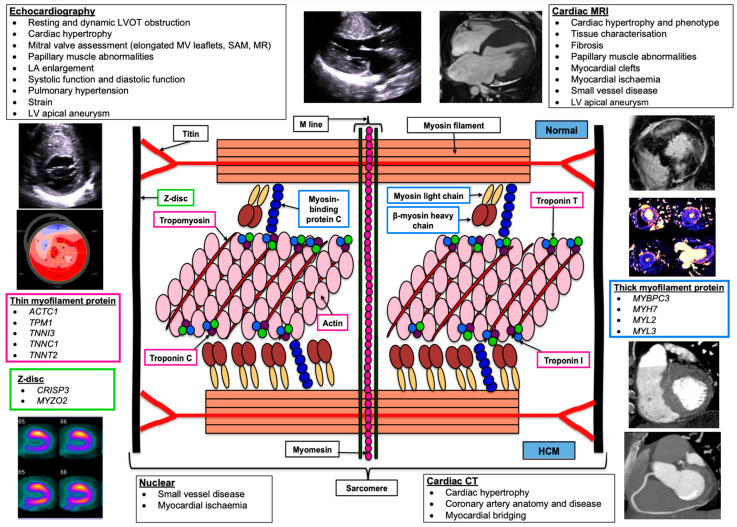
Hypertrophic cardiomyopathy (HCM) is characterized by abnormal growth of the myocardium with myofilament disarray and myocardial hyper-contractility, leading to left ventricular hypertrophy and fibrosis. Where culprit genes are identified, they typically relate to cardiomyocyte sarcomere structure and function. Multi-modality imaging plays a crucial role in the diagnosis, monitoring, and risk stratification of HCM, as well as in screening those at risk. Following the recent publication of the first European Society of Cardiology (ESC) cardiomyopathy guidelines, we build on previous reviews and explore the roles of electrocardiography, echocardiography, cardiac magnetic resonance (CMR), cardiac computed tomography (CT), and nuclear imaging. We examine each modality's strengths along with their limitations in turn, and discuss how they can be used in isolation, or in combination, to facilitate a personalized approach to patient care, as well as providing key information and robust safety and efficacy evidence within new areas of research.
Keywords: cardiac computed tomography; cardiac magnetic resonance imaging; echocardiography; hypertrophic cardiomyopathy; multi-modality imaging; nuclear imaging.
Conflict of interest statement
F.C.G. has no conflicts of interest to declare; M.M.Y.L. has received research grants through his institution, the University of Glasgow, from AstraZeneca and Boehringer Ingelheim and Roche Diagnostics, and is a member of a Trial Steering Committee for Cytokinetics and a Clinical Endpoints Committee for Bayer; C.J.C. is a member of a Steering Committee and has received advisory fees for Cytokinetics and speaker fees for Alnylam and Roche; S.N. has no conflicts of interest to declare.
Figures
References
-
- Arbelo E., Protonotarios A., Gimeno J.R., Arbustini E., Barriales-Villa R., Basso C., Bezzina C.R., Biagini E., Blom N.A., de Boer R.A., et al. 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC) Eur. Heart J. 2023;44:3503–3626. doi: 10.1093/eurheartj/ehad194. - DOI - PubMed
-
- Maron M.S., Link M.S., Udelson J.E., Kuvin J.T., Pandian N.G., Olivotto I., Nistri S., Cecchi F., Maron B.J., Zenovich A.G., et al. Hypertrophic Cardiomyopathy Is Predominantly a Disease of Left Ventricular Outflow Tract Obstruction. Circulation. 2006;114:2232–2239. doi: 10.1161/CIRCULATIONAHA.106.644682. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
