

Repeat Coronary Angiography in Patients Aged over 50 Years with Previously Normal/Non-Obstructive Coronary Angiogram-Insights from a Retrospective Study
- PMID: 38337564
- PMCID: PMC10855996
- DOI: 10.3390/jcm13030870
Repeat Coronary Angiography in Patients Aged over 50 Years with Previously Normal/Non-Obstructive Coronary Angiogram-Insights from a Retrospective Study
Abstract
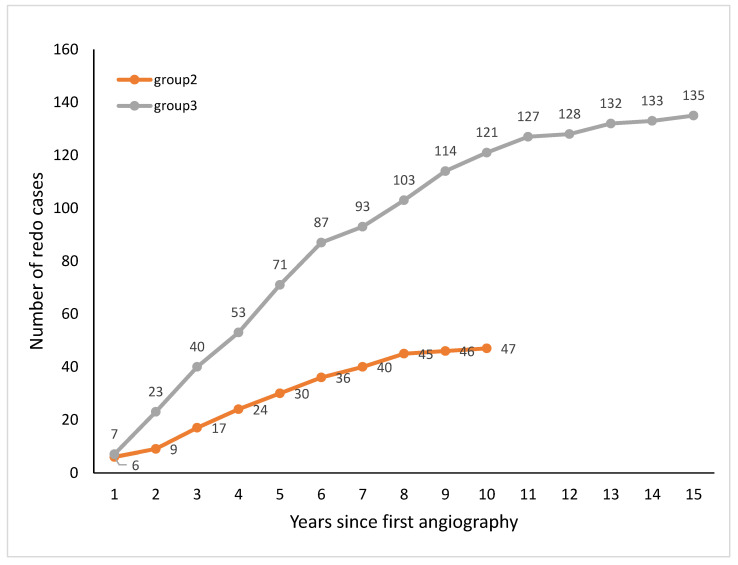
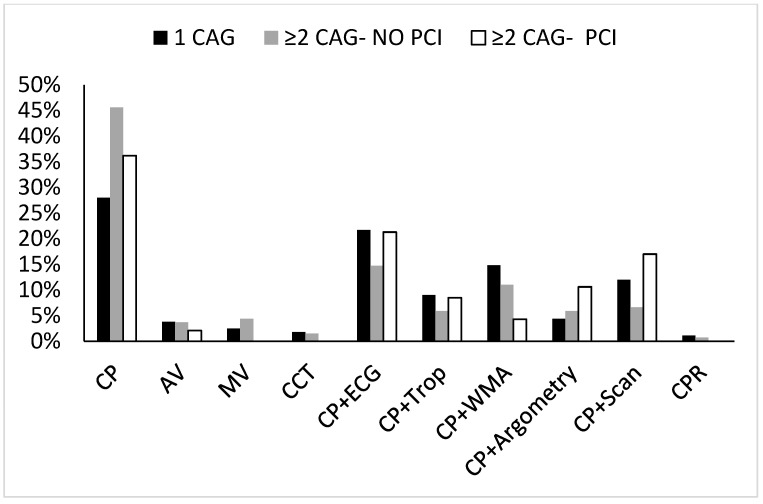
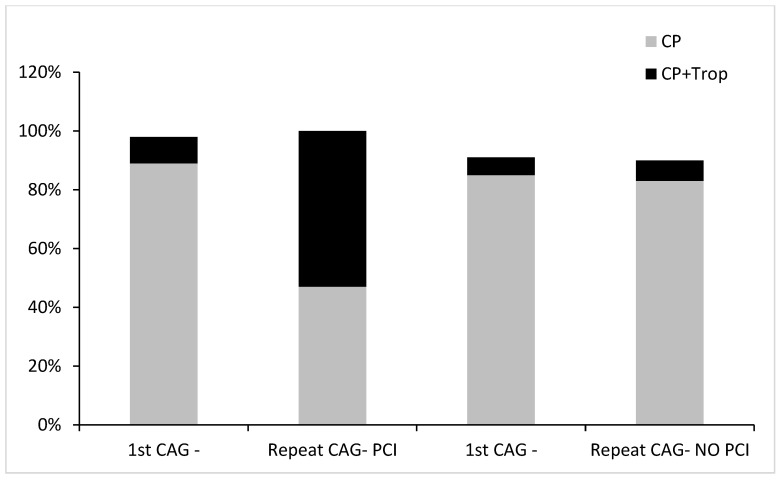
(1) Introduction: A significant proportion of patients undergoing coronary angiography (CAG) have normal (NCA) or non-obstructive coronary artery disease (NOCAD). This study retrospectively tested the incidence of re-catheterization, and long-term outcomes of this population in patients aged over 50 years. (2) Methods: We identified all patients above 50 years of age with NOCAD who underwent their first CAG at our center between January 2008 and December 2019. Patients were evaluated for their baseline characteristics, risk factors profile, and indication for CAG. Patients undergoing repeat CAG after the index procedure were assessed for the above, including the primary preventive pharmacotherapy prescribed. (3) Results: A total of 1939 patients were reported to have NOCAD. Of these, 1756 (90%) patients (62% males, median age 66 (56-75) years) had no repeat angiography (group 1). Repeat angiography was performed in 10%: 136 (7%) proved futile (median time for repeat angiography 5 (3-8) years) (group 3), and 47 (3%) ended with angioplasty (median time for repeat angiography 4 (3-6) years) (group 2). Male gender, BMI above 30 (23% vs. 13%), hypertension (68% vs. 57%), diabetes (28% vs. 17%) and smoking (36% vs. 19%) were significantly higher in the interventional group. Regression analysis showed both paroxysmal atrial fibrillation and hyperlipidemia were significantly associated with repeat CAG. The indication for the first CAG was mainly symptoms related. In the interventional repeat angiography (n = 47) the incidence of troponin positive cases increased from 8.2% before intervention to 57.5%, 50% being ST elevation cases. The symptoms-related cases went from 36.7% to 18.4%. Intriguingly, 85% of the interventional group were not prescribed statin and/or aspirin on a regular basis, and/or did not adhere to treatment. (4) Conclusions: NOCAD is a frequent occurrence. The threshold for repeat angiography must be higher, better reserved to troponin positive cases. Moreover, patients must be handled according to their risk profile, not being mistakenly reassured by a snapshot benign coronary angiography.
Keywords: atherosclerosis; atherothrombosis; myocardial infarction; non-significant coronary disease; normal angiogram.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Frequency, Etiology, and Impact of Unplanned Repeat Coronary Angiography After ST-Elevation Myocardial Infarction.Am J Cardiol. 2022 Jan 15;163:1-7. doi: 10.1016/j.amjcard.2021.09.038. Epub 2021 Nov 19. Am J Cardiol. 2022. PMID: 34809859
-
Clinical and electrocardiographic features of patients with myocardial infarction with non-obstructive coronary artery disease (MINOCA).J Cardiovasc Med (Hagerstown). 2021 Feb 1;22(2):104-109. doi: 10.2459/JCM.0000000000001027. J Cardiovasc Med (Hagerstown). 2021. PMID: 32706560
-
Impact of clinical presentation and presence of coronary sclerosis on long-term outcome of patients with non-obstructive coronary artery disease.BMC Cardiovasc Disord. 2018 Aug 22;18(1):173. doi: 10.1186/s12872-018-0908-z. BMC Cardiovasc Disord. 2018. PMID: 30134840 Free PMC article.
-
Association of Growth Differentiation Factor 15 with Arterial Stiffness and Endothelial Function in Subpopulations of Patients with Coronary Artery Disease: A Proof-of-Concept Study.Recent Adv Inflamm Allergy Drug Discov. 2022;16(2):107-115. doi: 10.2174/2772270817666221104120923. Recent Adv Inflamm Allergy Drug Discov. 2022. PMID: 36336806
-
Predictors of Obstructive Sleep Apnoea (OSA) Population in the Coronary Angiogram Database of South Australia (CADOSA).Curr Probl Cardiol. 2022 Jun;47(6):100846. doi: 10.1016/j.cpcardiol.2021.100846. Epub 2021 Mar 20. Curr Probl Cardiol. 2022. PMID: 33994030 Review.
References
-
- Shaw L.J., Shaw R.E., Merz C.N.B., Brindis R.G., Klein L.W., Nallamothu B., Douglas P.S., Krone R.J., McKay C.R., Block P.C., et al. Impact of Ethnicity and Gender Differences on Angiographic Coronary Artery Disease Prevalence and In-Hospital Mortality in the American College of Cardiology–National Cardiovascular Data Registry. Circulation. 2008;117:1787–1801. doi: 10.1161/CIRCULATIONAHA.107.726562. - DOI - PubMed
LinkOut - more resources
Full Text Sources
