

Maternal Diet Associates with Offspring Bone Mineralization, Fracture Risk and Enamel Defects in Childhood and Influences the Prenatal Effect of High-Dose Vitamin D Supplementation
- PMID: 38337692
- PMCID: PMC10856831
- DOI: 10.3390/nu16030405
Maternal Diet Associates with Offspring Bone Mineralization, Fracture Risk and Enamel Defects in Childhood and Influences the Prenatal Effect of High-Dose Vitamin D Supplementation
Abstract
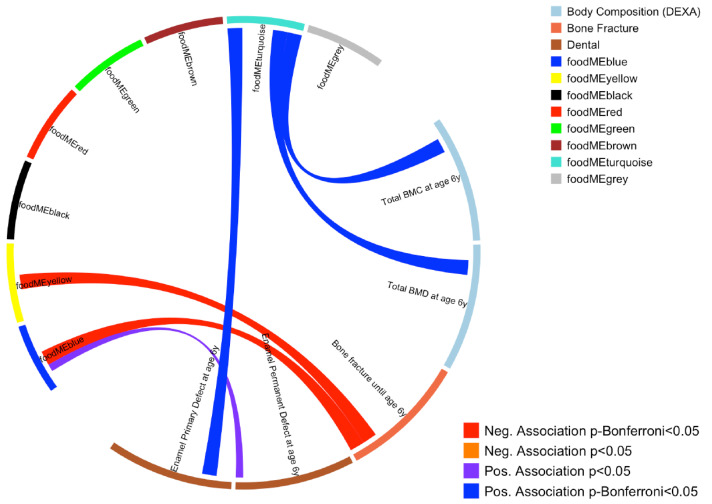
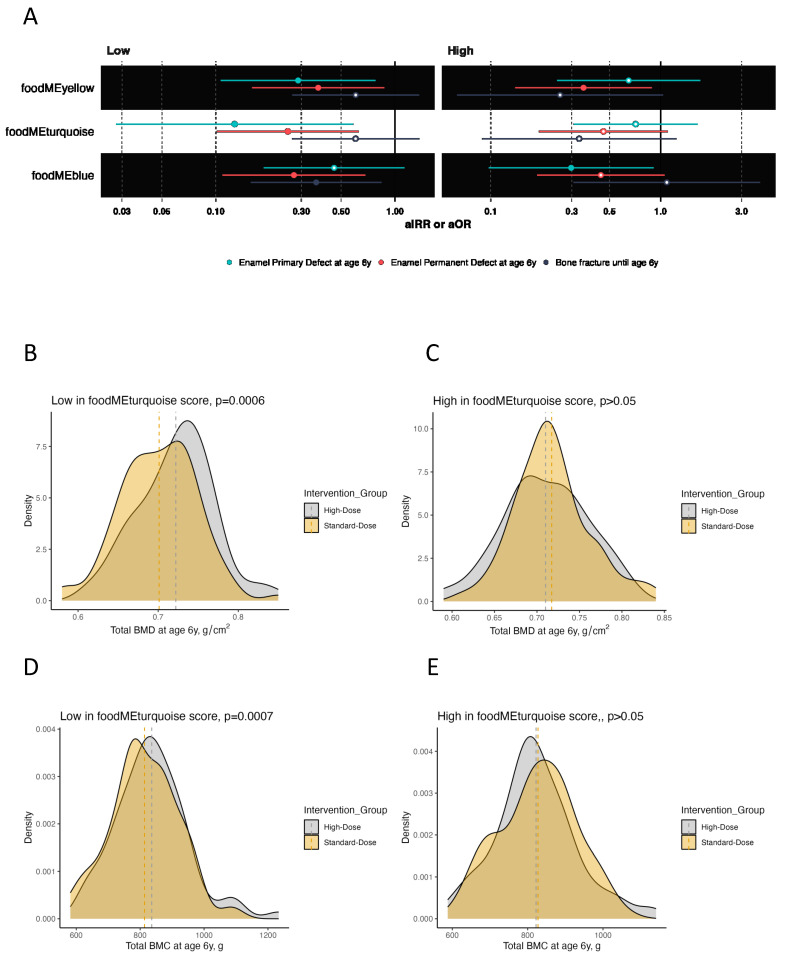
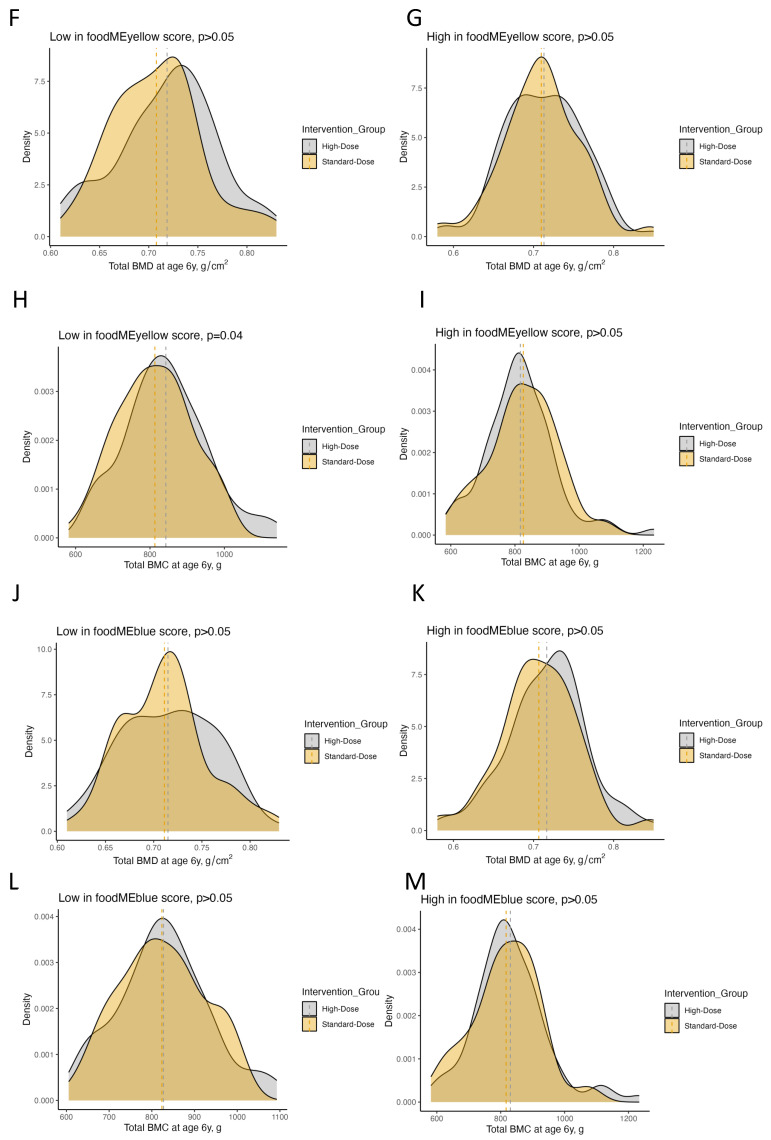
We previously demonstrated a beneficial effect of high-dose vitamin D in pregnancy on offspring bone and dental health. Here, we investigated the effect of maternal dietary patterns during pregnancy on the risk of bone fractures, bone mineralization and enamel defects until age 6 years in the offspring. Further, the influence of diet on the effect of high-dose vitamin D was analyzed in the COPSAC2010 mother-child cohort including 623 mother-child pairs. A weighted network analysis on FFQs revealed three specific maternal dietary patterns that associated (Bonferroni p < 0.05) with both offspring bone and dental health. The effect of prenatal high-dose (2800 IU/day) vs. standard-dose (400 IU/day) vitamin D on offspring bone mineral content (adjusted mean difference (aMD): 33.29 g, 95% CI: 14.48-52.09, p < 0.001), bone mineral density (aMD: 0.02 g/cm2 (0.01-0.04), p < 0.001), fracture risk (adjusted incidence rate ratio: 0.36 (0.16-0.84), p = 0.02), and enamel defects in primary (adjusted odds ratio (aOR): 0.13 (0.03-0.58), p < 0.01) and permanent molars (aOR: 0.25; (0.10-0.63), p < 0.01) was most pronounced when mothers had lower intake of fruit, vegetables, meat, eggs, sweets, whole grain, offal and fish. This study suggests that prenatal dietary patterns influence offspring bone and dental development, and should be considered in order to obtain the full benefits of vitamin D to enhance personalized supplementation strategy.
Keywords: bone health; dental health; pregnancy diet; vitamin D.
Conflict of interest statement
All authors declare no potential, perceived, or real conflicts of interest regarding the content of this manuscript.
Figures
References
-
- Schroth R.J., Christensen J., Morris M., Gregory P., Mittermuller B.A., Rockman-Greenberg C. The Influence of Prenatal Vitamin D Supplementation on Dental Caries in Infants. J. Can. Dent. Assoc. 2020;86:k13. - PubMed
-
- van der Tas J.T., Elfrink M.E.C., Heijboer A.C., Rivadeneira F., Jaddoe V.W.V., Tiemeier H., Schoufour J.D., Moll H.A., Ongkosuwito E.M., Wolvius E.B., et al. Foetal, neonatal and child vitamin D status and enamel hypomineralization. Community Dent. Oral. Epidemiol. 2018;46:343–351. doi: 10.1111/cdoe.12372. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
