

Molecular Genetic Profile of Myelofibrosis: Implications in the Diagnosis, Prognosis, and Treatment Advancements
- PMID: 38339265
- PMCID: PMC10854658
- DOI: 10.3390/cancers16030514
Molecular Genetic Profile of Myelofibrosis: Implications in the Diagnosis, Prognosis, and Treatment Advancements
Abstract
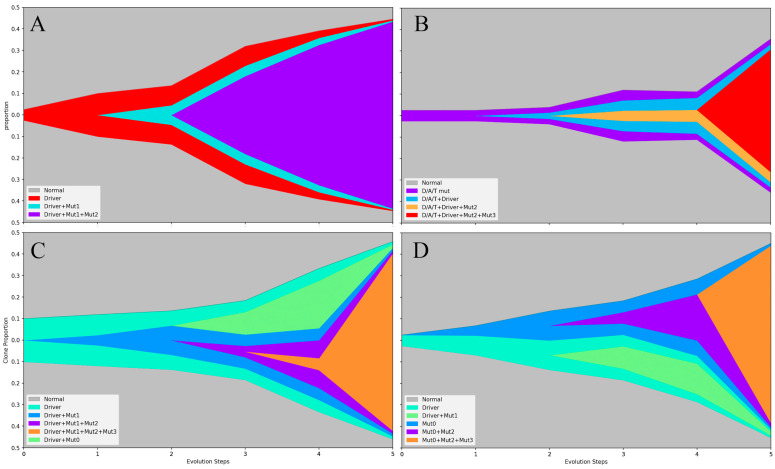
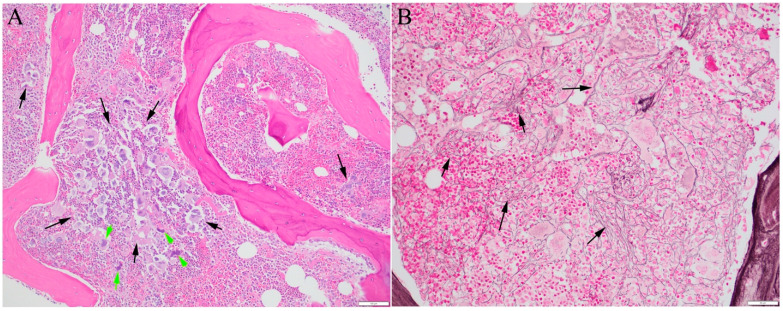
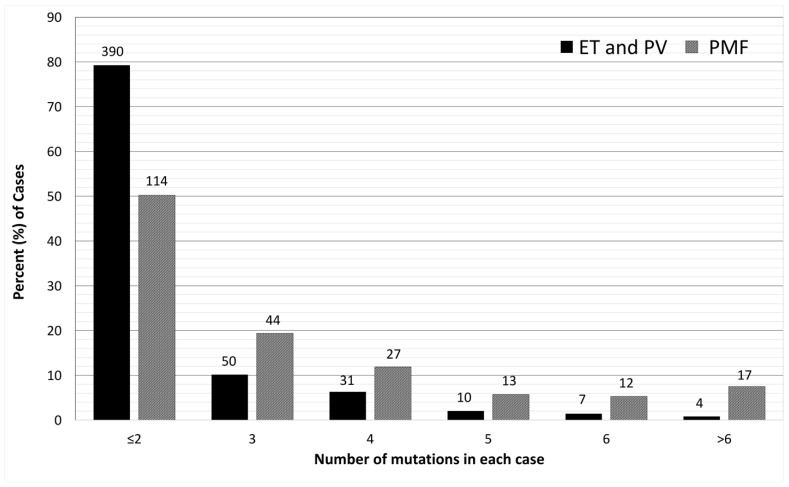
Myelofibrosis (MF) is an essential element of primary myelofibrosis, whereas secondary MF may develop in the advanced stages of other myeloid neoplasms, especially polycythemia vera and essential thrombocythemia. Over the last two decades, advances in molecular diagnostic techniques, particularly the integration of next-generation sequencing in clinical laboratories, have revolutionized the diagnosis, classification, and clinical decision making of myelofibrosis. Driver mutations involving JAK2, CALR, and MPL induce hyperactivity in the JAK-STAT signaling pathway, which plays a central role in cell survival and proliferation. Approximately 80% of myelofibrosis cases harbor additional mutations, frequently in the genes responsible for epigenetic regulation and RNA splicing. Detecting these mutations is crucial for diagnosing myeloproliferative neoplasms (MPNs), especially in cases where no mutations are present in the three driver genes (triple-negative MPNs). While fibrosis in the bone marrow results from the disturbance of inflammatory cytokines, it is fundamentally associated with mutation-driven hematopoiesis. The mutation profile and order of acquiring diverse mutations influence the MPN phenotype. Mutation profiling reveals clonal diversity in MF, offering insights into the clonal evolution of neoplastic progression. Prognostic prediction plays a pivotal role in guiding the treatment of myelofibrosis. Mutation profiles and cytogenetic abnormalities have been integrated into advanced prognostic scoring systems and personalized risk stratification for MF. Presently, JAK inhibitors are part of the standard of care for MF, with newer generations developed for enhanced efficacy and reduced adverse effects. However, only a minority of patients have achieved a significant molecular-level response. Clinical trials exploring innovative approaches, such as combining hypomethylation agents that target epigenetic regulators, drugs proven effective in myelodysplastic syndrome, or immune and inflammatory modulators with JAK inhibitors, have demonstrated promising results. These combinations may be more effective in patients with high-risk mutations and complex mutation profiles. Expanding mutation profiling studies with more sensitive and specific molecular methods, as well as sequencing a broader spectrum of genes in clinical patients, may reveal molecular mechanisms in cases currently lacking detectable driver mutations, provide a better understanding of the association between genetic alterations and clinical phenotypes, and offer valuable information to advance personalized treatment protocols to improve long-term survival and eradicate mutant clones with the hope of curing MF.
Keywords: JAK inhibitor; epigenetic regulation; molecular diagnostics; mutations; myelofibrosis; myeloproliferative neoplasm; next-generation sequencing; primary myelofibrosis.
Conflict of interest statement
Nikolaos Papadantonakis reports honoraria from Agios Pharmaceuticals and CTI Biopharma. He participated in advisory boards for Agios Pharmaceuticals and CTI Biopharma. He received research grants (paid to the institution) from Gilead, ONO PHARMA USA, and Abbvie. The rest of the authors have no conflicts of interest to declare.
Figures
References
-
- Khoury J.D., Solary E., Abla O., Akkari Y., Alaggio R., Apperley J.F., Bejar R., Berti E., Busque L., Chan J.K.C., et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and histiocytic/Dendritic neoplasms. Leukemia. 2022;36:1703–1719. doi: 10.1038/s41375-022-01613-1. - DOI - PMC - PubMed
-
- Arber D.A., Orazi A., Hasserjian R.P., Borowitz M.J., Calvo K.R., Kvasnicka H.-M., Wang S.A., Bagg A., Barbui T., Branford S., et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating morphologic, clinical, and genomic data. Blood. 2022;140:1200–1228. doi: 10.1182/blood.2022015850. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
