

The Feasibility and Accuracy of Holographic Navigation with Laser Crosshair Simulator Registration on a Mixed-Reality Display
- PMID: 38339612
- PMCID: PMC10857152
- DOI: 10.3390/s24030896
The Feasibility and Accuracy of Holographic Navigation with Laser Crosshair Simulator Registration on a Mixed-Reality Display
Abstract
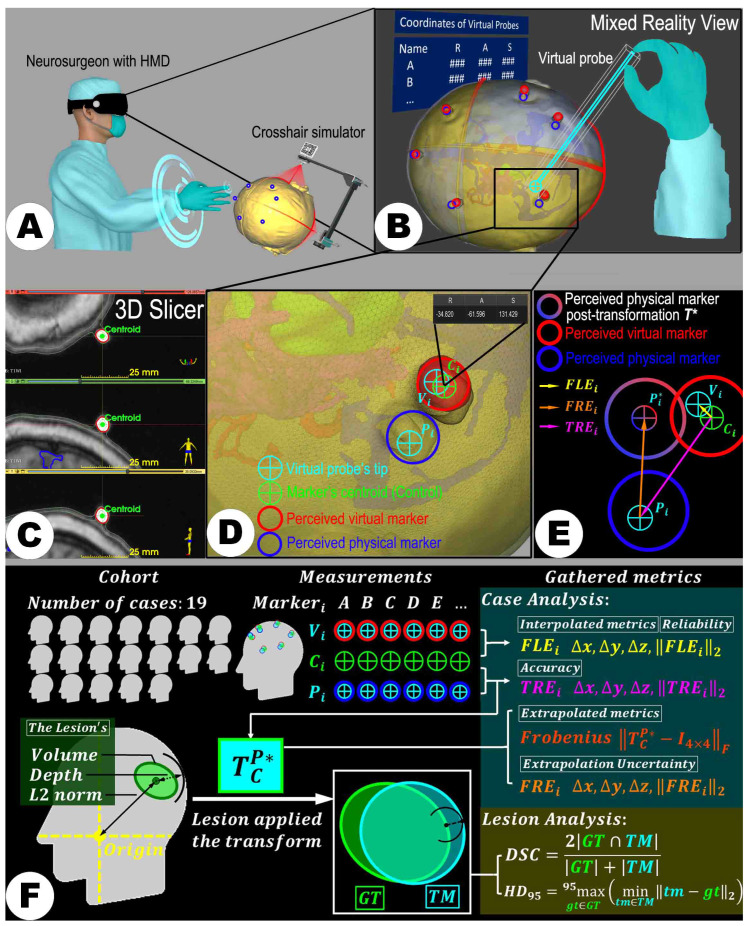
Addressing conventional neurosurgical navigation systems' high costs and complexity, this study explores the feasibility and accuracy of a simplified, cost-effective mixed reality navigation (MRN) system based on a laser crosshair simulator (LCS). A new automatic registration method was developed, featuring coplanar laser emitters and a recognizable target pattern. The workflow was integrated into Microsoft's HoloLens-2 for practical application. The study assessed the system's precision by utilizing life-sized 3D-printed head phantoms based on computed tomography (CT) or magnetic resonance imaging (MRI) data from 19 patients (female/male: 7/12, average age: 54.4 ± 18.5 years) with intracranial lesions. Six to seven CT/MRI-visible scalp markers were used as reference points per case. The LCS-MRN's accuracy was evaluated through landmark-based and lesion-based analyses, using metrics such as target registration error (TRE) and Dice similarity coefficient (DSC). The system demonstrated immersive capabilities for observing intracranial structures across all cases. Analysis of 124 landmarks showed a TRE of 3.0 ± 0.5 mm, consistent across various surgical positions. The DSC of 0.83 ± 0.12 correlated significantly with lesion volume (Spearman rho = 0.813, p < 0.001). Therefore, the LCS-MRN system is a viable tool for neurosurgical planning, highlighting its low user dependency, cost-efficiency, and accuracy, with prospects for future clinical application enhancements.
Keywords: augmented reality; automatic registration; dice similarity coefficient; head phantom; intracranial lesion; laser crosshair simulator; mixed reality; neuronavigation; neurosurgical planning; target registration error.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures









References
-
- Stieglitz L.H., Fichtner J., Andres R., Schucht P., Krähenbühl A.K., Raabe A., Beck J. The silent loss of neuronavigation accuracy: A systematic retrospective analysis of factors influencing the mismatch of frameless stereotactic systems in cranial neurosurgery. Neurosurgery. 2013;72:796–807. doi: 10.1227/NEU.0b013e318287072d. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
