

Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy to Treat Pseudomyxoma Peritonei of Ovarian Origin: A Retrospective French RENAPE Group Study
- PMID: 38341381
- PMCID: PMC10997733
- DOI: 10.1245/s10434-023-14850-0
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy to Treat Pseudomyxoma Peritonei of Ovarian Origin: A Retrospective French RENAPE Group Study
Abstract
Background: Ovarian pseudomyxoma peritonei (OPMP) are rare, without well-defined therapeutic guidelines. We aimed to evaluate cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) to treat OPMP.
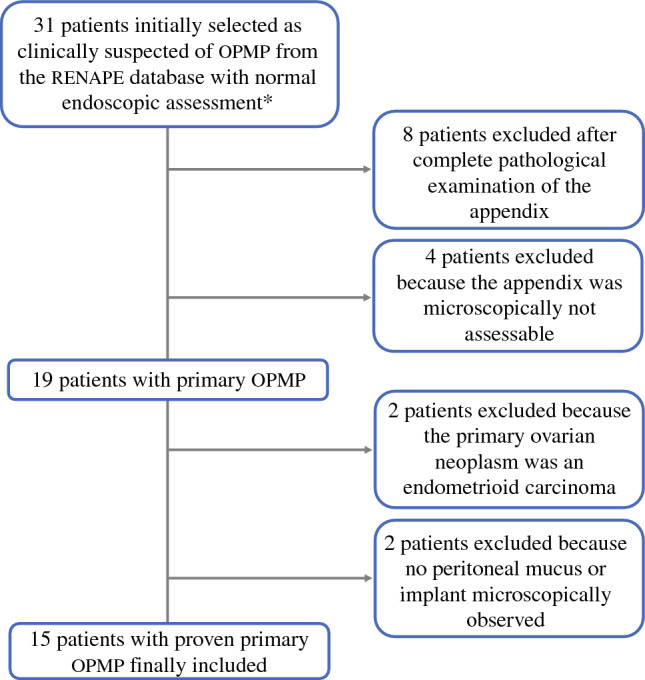
Methods: Patients from the French National Network for Rare Peritoneal Tumors (RENAPE) database with proven OPMP treated by CRS/HIPEC and with histologically normal appendix and digestive endoscopy were retrospectively included. Clinical and follow-up data were collected. Histopathological and immunohistochemical features were reviewed.
Results: Fifteen patients with a median age of 56 years were included. The median Peritoneal Cancer Index was 16. Following CRS, the completeness of cytoreduction (CC) score was CC-0 for 9/15 (60%) patients, CC-1 for 5/15 (33.3%) patients, and CC-2 for 1/15 (6.7%) patients. The median tumor size was 22.5 cm. After pathological review and immunohistochemical studies, tumors were classified as Group 1 (mucinous ovarian epithelial neoplasms) in 3/15 (20%) patients; Group 2 (mucinous neoplasm in ovarian teratoma) in 4/15 (26.7%) patients; Group 3 (mucinous neoplasm probably arising in ovarian teratoma) in 5/15 (33.3%) patients; and Group 4 (non-specific group) in 3/15 (20%) patients. Peritoneal lesions were OPMP pM1a/acellular, pM1b/grade 1 (hypocellular) and pM1b/grade 3 (signet-ring cells) in 13/15 (86.7%), 1/15 (6.7%) and 1/15 (6.7%) patients, respectively. Disease-free survival analysis showed a difference (p = 0.0463) between OPMP with teratoma/likely-teratoma origin (groups 2 and 3; 100% at 1, 5, and 10 years), and other groups (groups 1 and 4; 100%, 66.6%, and 50% at 1, 5, and 10 years, respectively).
Conclusion: These results suggested that a primary therapeutic strategy using complete CRS/HIPEC for patients with OPMP led to favorable long-term outcomes.
Keywords: Cytoreduction; HIPEC; Mucinous tumor from teratoma; Ovarian carcinoma; Ovarian pseudomyxoma; Peritoneal pseudomyxoma.
© 2024. The Author(s).
Conflict of interest statement
Olivier Glehen is a consultant for Gamida. Alexis Trecourt, Naoual Bakrin, Witold Gertych, Laurent Villeneuve, Sylvie Isaac, Nazim Benzerdjeb, Juliette Fontaine, Catherine Genestie, Peggy Dartigues, Agnès Leroux, François Quenet, Frederic Marchal, Cecile Odin, Lakhdar Khellaf, Magali Svrcek, Sixte Thierry, Marilyn Augros, Alhadeedi Omar, Mojgan Devouassoux-Shisheboran, and Vahan Kepenekian have no conflicts of interest to declare in relation to this work.
Figures




References
-
- Ronnett BM, Zahn CM, Kurman RJ, Kass ME, Sugarbaker PH, Shmookler BM. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol. 1995;19(12):1390–1408. doi: 10.1097/00000478-199512000-00006. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
