

A novel theta-controlled vibrotactile brain-computer interface to treat chronic pain: a pilot study
- PMID: 38341457
- PMCID: PMC10858946
- DOI: 10.1038/s41598-024-53261-3
A novel theta-controlled vibrotactile brain-computer interface to treat chronic pain: a pilot study
Abstract
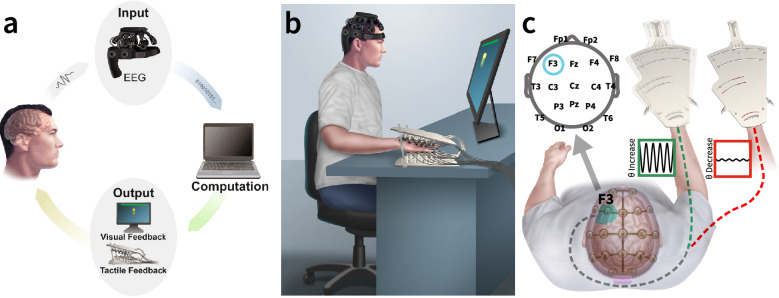
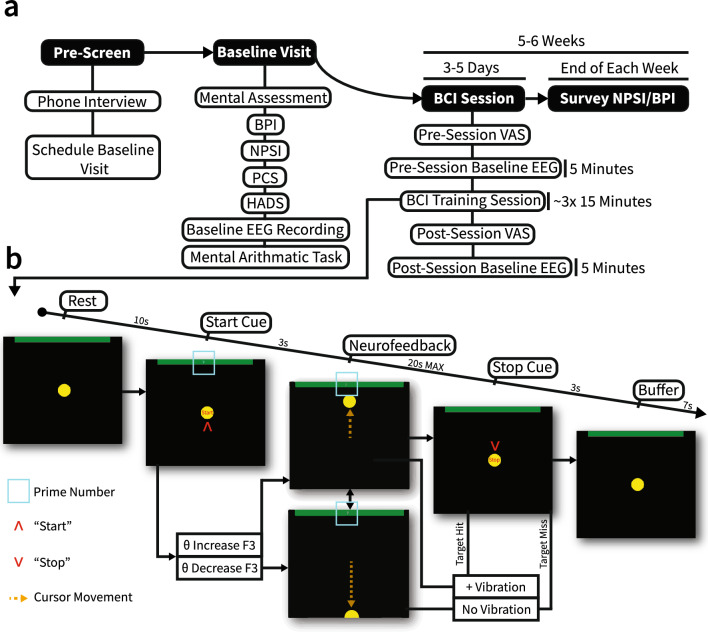
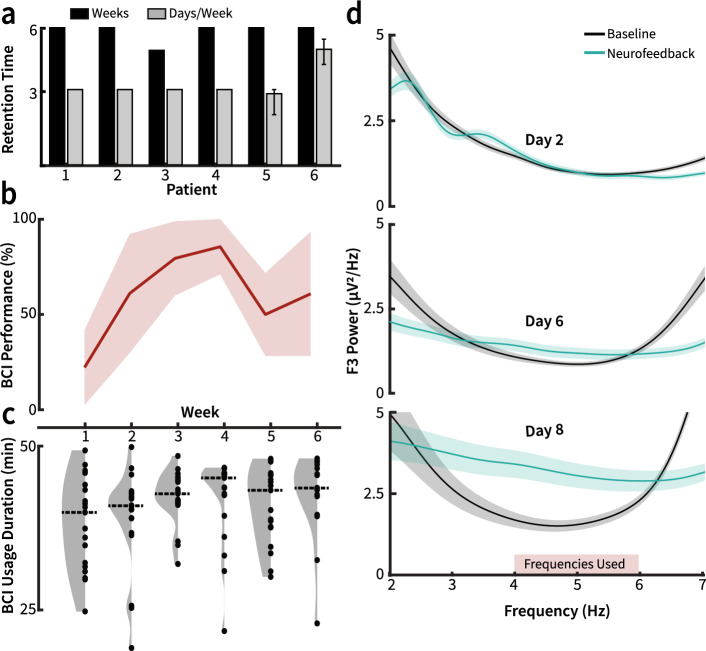
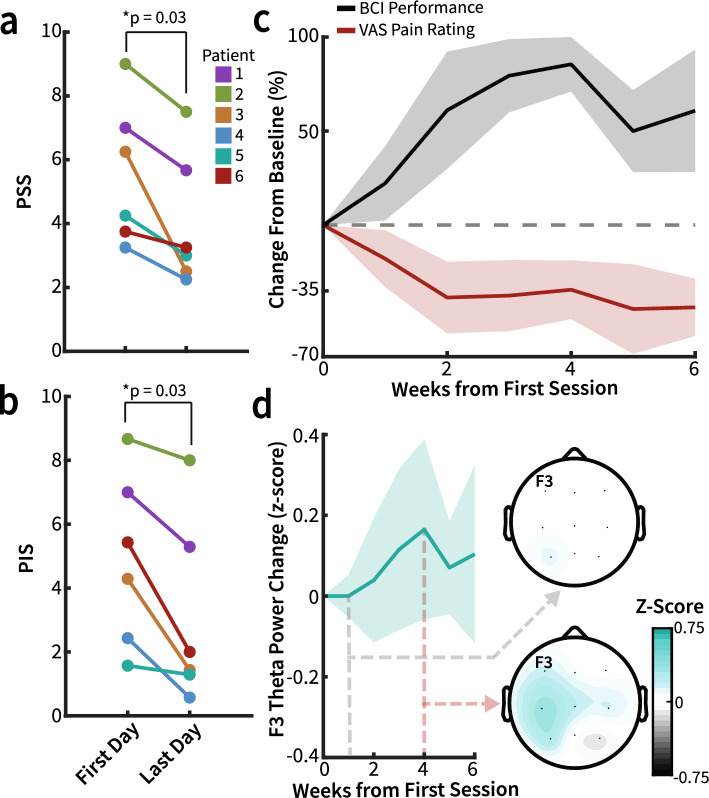
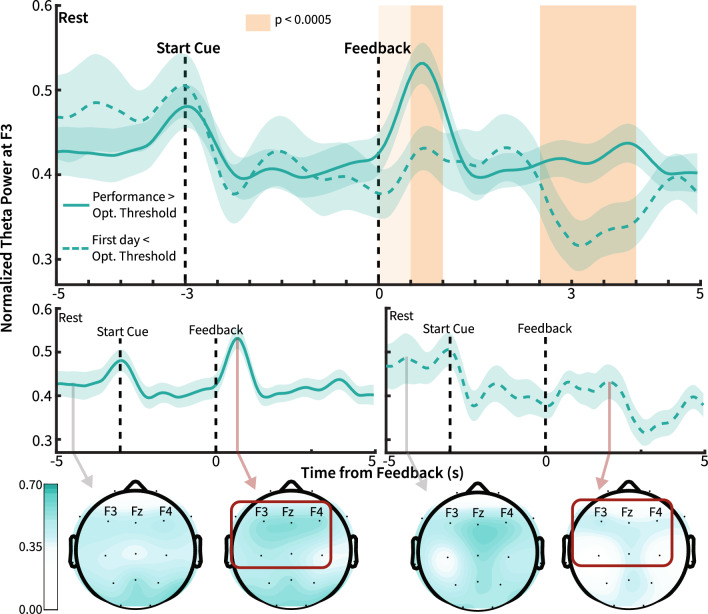
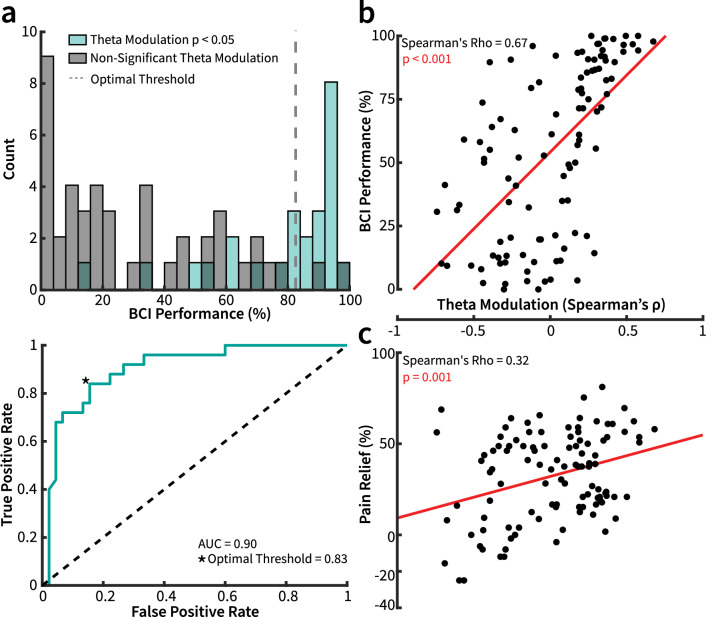
Limitations in chronic pain therapies necessitate novel interventions that are effective, accessible, and safe. Brain-computer interfaces (BCIs) provide a promising modality for targeting neuropathology underlying chronic pain by converting recorded neural activity into perceivable outputs. Recent evidence suggests that increased frontal theta power (4-7 Hz) reflects pain relief from chronic and acute pain. Further studies have suggested that vibrotactile stimulation decreases pain intensity in experimental and clinical models. This longitudinal, non-randomized, open-label pilot study's objective was to reinforce frontal theta activity in six patients with chronic upper extremity pain using a novel vibrotactile neurofeedback BCI system. Patients increased their BCI performance, reflecting thought-driven control of neurofeedback, and showed a significant decrease in pain severity (1.29 ± 0.25 MAD, p = 0.03, q = 0.05) and pain interference (1.79 ± 1.10 MAD p = 0.03, q = 0.05) scores without any adverse events. Pain relief significantly correlated with frontal theta modulation. These findings highlight the potential of BCI-mediated cortico-sensory coupling of frontal theta with vibrotactile stimulation for alleviating chronic pain.
© 2024. The Author(s).
Conflict of interest statement
The study was supported, in part, by start-up funding from Washington University Department of Anesthesiology to Simon Haroutounian. This work was also supported by the National Institutes of Health (NIH) grants R01-EB026439, U24-NS109103, P41-EB018783, and Fondazione Neurone. Simon Haroutounian has received in the past 36 months research grants and contracts from the US National Institutes of Health, US Department of Defense, Patient-Centered Outcomes Research Institute and Eli Lilly, and personal fees from Vertex Pharmaceuticals, Rafa Laboratories and GW Pharma, outside the scope of submitted work. Eric Leuthardt has stock ownership in Neurolutions, Osteovantage, Face to Face Biometrics, Caeli Vascular, Acera, Sora Neuroscience, Inner Cosmos, Kinetrix, NeuroDev, Inflexion Vascular, Aurenar, and Petal Surgical. He is a consultant for E15, Neurolutions, Inc., and Petal Surgical. Washington University owns equity in Neurolutions. All other authors do not report any conflicts of interest.
Figures
Similar articles
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
Acupuncture for neuropathic pain in adults.Cochrane Database Syst Rev. 2017 Dec 2;12(12):CD012057. doi: 10.1002/14651858.CD012057.pub2. Cochrane Database Syst Rev. 2017. PMID: 29197180 Free PMC article.
-
Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews.Cochrane Database Syst Rev. 2017 Apr 24;4(4):CD011279. doi: 10.1002/14651858.CD011279.pub3. Cochrane Database Syst Rev. 2017. PMID: 28436583 Free PMC article.
-
Gabapentin for chronic neuropathic pain and fibromyalgia in adults.Cochrane Database Syst Rev. 2014 Apr 27;2014(4):CD007938. doi: 10.1002/14651858.CD007938.pub3. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2017 Jun 09;6:CD007938. doi: 10.1002/14651858.CD007938.pub4. PMID: 24771480 Free PMC article. Updated.
-
The analgesic effect of electroencephalographic neurofeedback for people with chronic pain: A systematic review and meta-analysis.Eur J Neurol. 2022 Mar;29(3):921-936. doi: 10.1111/ene.15189. Epub 2021 Dec 10. Eur J Neurol. 2022. PMID: 34813662
Cited by
-
Evaluating the effectiveness of neurofeedback in chronic pain management: a narrative review.Front Psychol. 2024 May 6;15:1369487. doi: 10.3389/fpsyg.2024.1369487. eCollection 2024. Front Psychol. 2024. PMID: 38770259 Free PMC article. Review.
-
A Comprehensive Survey of Brain-Computer Interface Technology in Health care: Research Perspectives.J Med Signals Sens. 2025 Jun 9;15:16. doi: 10.4103/jmss.jmss_49_24. eCollection 2025. J Med Signals Sens. 2025. PMID: 40546334 Free PMC article. Review.
-
Neural functional rehabilitation: Exploring neuromuscular reconstruction technology advancements and challenges.Neural Regen Res. 2026 Jan 1;21(1):173-186. doi: 10.4103/NRR.NRR-D-24-00613. Epub 2024 Dec 7. Neural Regen Res. 2026. PMID: 39665789 Free PMC article.
-
Cortical spectral dynamics of vibrotactile frequency processing.Sci Rep. 2025 Aug 14;15(1):29847. doi: 10.1038/s41598-025-14870-8. Sci Rep. 2025. PMID: 40813878 Free PMC article.
-
Closed-loop neural interfaces for pain: Where do we stand?Cell Rep Med. 2024 Oct 15;5(10):101662. doi: 10.1016/j.xcrm.2024.101662. Cell Rep Med. 2024. PMID: 39413730 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
