

This is a preprint.
SARS-CoV-2 vaccination in the first year after hematopoietic cell transplant or chimeric antigen receptor T cell therapy: A prospective, multicenter, observational study (BMT CTN 2101)
- PMID: 38343800
- PMCID: PMC10854344
- DOI: 10.1101/2024.01.24.24301058
SARS-CoV-2 vaccination in the first year after hematopoietic cell transplant or chimeric antigen receptor T cell therapy: A prospective, multicenter, observational study (BMT CTN 2101)
Update in
-
SARS-CoV-2 Vaccination in the First Year After Hematopoietic Cell Transplant or Chimeric Antigen Receptor T-Cell Therapy: A Prospective, Multicenter, Observational Study.Clin Infect Dis. 2024 Aug 16;79(2):542-554. doi: 10.1093/cid/ciae291. Clin Infect Dis. 2024. PMID: 38801746 Free PMC article.
Abstract
Background: The optimal timing of vaccination with SARS-CoV-2 vaccines after cellular therapy is incompletely understood.
Objective: To describe humoral and cellular responses after SARS-CoV-2 vaccination initiated <4 months versus 4-12 months after cellular therapy.
Design: Multicenter prospective observational study.
Setting: 34 centers in the United States.
Participants: 466 allogeneic hematopoietic cell transplant (HCT; n=231), autologous HCT (n=170), or chimeric antigen receptor T cell (CAR-T cell) therapy (n=65) recipients enrolled between April 2021 and June 2022.
Interventions: SARS-CoV-2 vaccination as part of routine care.
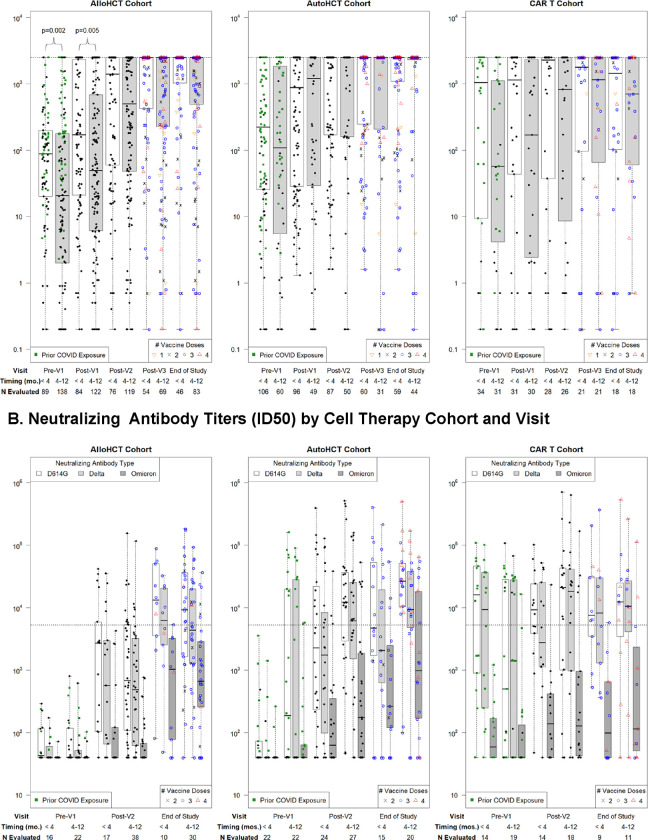
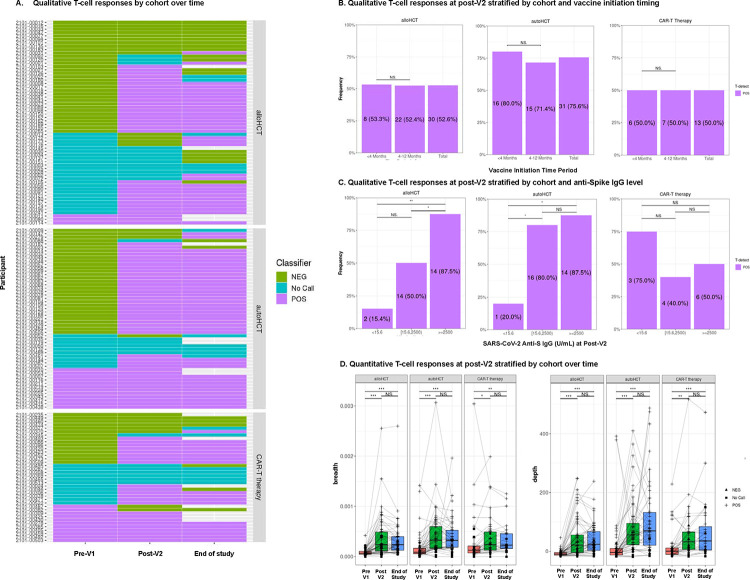
Measurements: We obtained blood prior to and after vaccinations at up to five time points and tested for SARS-CoV-2 spike (anti-S) IgG in all participants and neutralizing antibodies for Wuhan D614G, Delta B.1.617.2, and Omicron B.1.1.529 strains, as well as SARS-CoV-2-specific T cell receptors (TCRs), in a subgroup.
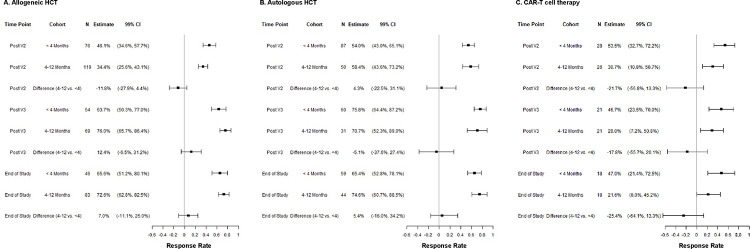
Results: Anti-S IgG and neutralizing antibody responses increased with vaccination in HCT recipients irrespective of vaccine initiation timing but were unchanged in CAR-T cell recipients initiating vaccines within 4 months. Anti-S IgG ≥2,500 U/mL was correlated with high neutralizing antibody titers and attained by the last time point in 70%, 69%, and 34% of allogeneic HCT, autologous HCT, and CAR-T cell recipients, respectively. SARS-CoV-2-specific T cell responses were attained in 57%, 83%, and 58%, respectively. Humoral and cellular responses did not significantly differ among participants initiating vaccinations <4 months vs 4-12 months after cellular therapy. Pre-cellular therapy SARS-CoV-2 infection or vaccination were key predictors of post-cellular therapy anti-S IgG levels.
Limitations: The majority of participants were adults and received mRNA vaccines.
Conclusions: These data support starting mRNA SARS-CoV-2 vaccination three to four months after allogeneic HCT, autologous HCT, and CAR-T cell therapy.
Funding: National Marrow Donor Program, Leukemia and Lymphoma Society, Multiple Myeloma Research Foundation, Novartis, LabCorp, American Society for Transplantation and Cellular Therapy, Adaptive Biotechnologies, and the National Institutes of Health.
Keywords: Covid-19; SARS-CoV-2; hematopoietic cell transplant; transplant; vaccine.
Conflict of interest statement
Declarations of interest J.A.H: Research funding: AlloVir, Geovax, Merck; Consulting: Pfizer, Gilead, Moderna, Geovax, AlloVir. J-A.H.Y.: Research funding: AlloVir, Ansun, Cidara, F2G, GSK, NobelPharma, Pulmocide, Scynexis, Shire/Takeda L.W.L: Employment and equity holder in Adaptive Biotechnologies Corp. M.V.D.: Research funding: Janssen, Roche/Genentech R.N.: Consulting: Ono Pharmaceutical, Jazz Pharmaceuticals, BluebirdBio, Omeros Pharmaceutical, Sanofi, Pfizer J. M.: Consulting: Evision, Kite, Allovir, Bristol Myers Squibb, Novartis, CRISPR, Nektar, Caribiou Bio, Sana Technologies, Legend Biotech S.D.W.: Research funding: MSK Leukemia SPORE Career Enhancement Program and MSK Gerstner Physician Scholar program J.J.A.: Employment: National Marrow Donor Program. Advisory Board: AscellaHealth, Takeda M. H.: Research Support/Funding: Takeda Pharmaceutical Company; ADC Therapeutics; Spectrum Pharmaceuticals; Astellas Pharma. Consultancy: Incyte Corporation, MorphoSys, SeaGen, Gamida Cell, Novartis, Legend Biotech, Kadmon, ADC Therapeutics; Omeros, Abbvie, Caribou, CRISPR, Genmab, Kite. Speaker’s Bureau: Sanofi Genzyme, AstraZeneca, BeiGene, ADC Therapeutics, Kite. DMC: Myeloid Therapeutics, Inc M.L.R.: Research funding from Jazz Pharmaceuticals and Atara Bio-Pharma. Employment by IQVIA Biotech and Kura Oncology. Stock in Kura Oncology. M.M.H. Research funding from Astellas Pharma, CSL Behring, Incyte, Sanofi. Consultancy: Sobi, Inc. M-A.P.: Honoraria from Adicet, Allogene, Allovir, Caribou Biosciences, Celgene, Bristol-Myers Squibb, Equilium, Exevir, ImmPACT Bio, Incyte, Karyopharm, Kite/Gilead, Merck, Miltenyi Biotec, MorphoSys, Nektar Therapeutics, Novartis, Omeros, OrcaBio, Sanofi, Syncopation, VectivBio AG, and Vor Biopharma. He serves on DSMBs for Cidara Therapeutics and Sellas Life Sciences, and the scientific advisory board of NexImmune. He has ownership interests in NexImmune, Omeros and OrcaBio. He has received institutional research support for clinical trials from Allogene, Incyte, Kite/Gilead, Miltenyi Biotec, Nektar Therapeutics, and Novartis. All other authors report no relevant conflicts of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous