

Critical Case of a Preterm Infant Infected With Respiratory Syncytial Virus Managed in the Pediatric Intensive Care Unit: A Case Report
- PMID: 38344580
- PMCID: PMC10858791
- DOI: 10.7759/cureus.52119
Critical Case of a Preterm Infant Infected With Respiratory Syncytial Virus Managed in the Pediatric Intensive Care Unit: A Case Report
Abstract
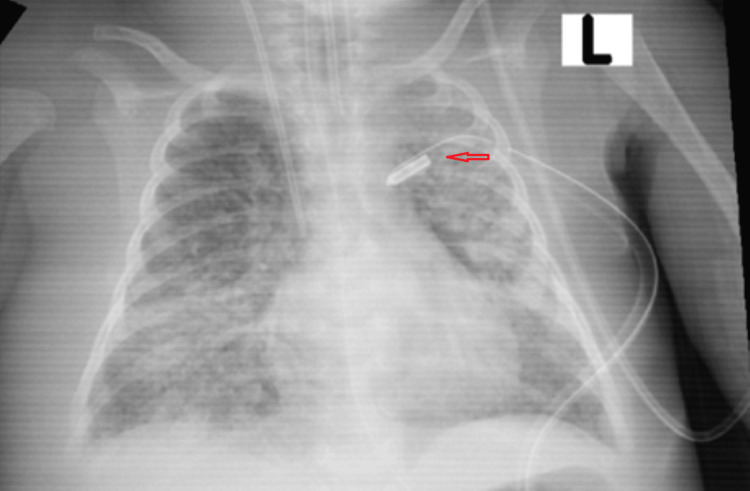
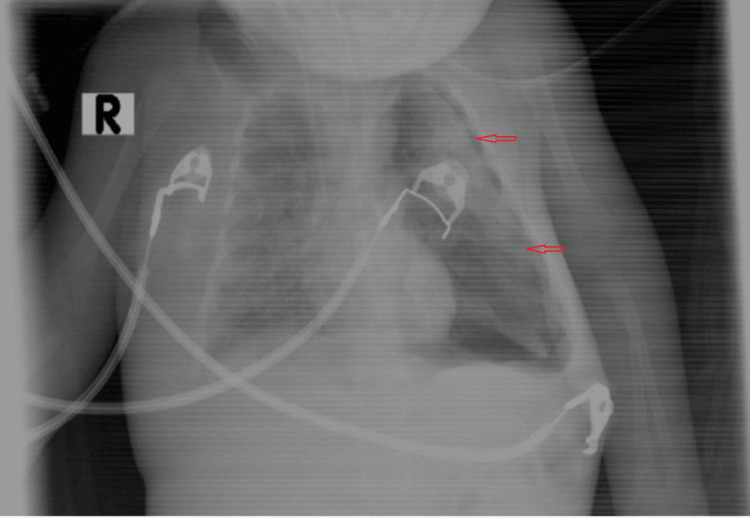
We describe a critical case of a respiratory syncytial virus (RSV) infection in a preterm infant resulting in respiratory failure with advanced respiratory interventions and discharge from our hospital without the requirement for home oxygen therapy or tube feeding. The infant, delivered at 35 weeks gestation due to a premature rupture of the membranes with a birth weight of 2 kg, initially demonstrated a stable postnatal course. The baby required no resuscitation, with Apgar scores of 8 and 9 at one and five minutes, respectively. The infant was discharged in good condition after four days of hospitalization. This report presents a critical case of RSV infection in a preterm infant requiring intensive care. The infant, born at 35 weeks gestation, initially appeared healthy but developed severe symptoms at 22 days old. The emergency evaluation revealed significant respiratory distress and confirmed RSV pneumonia. Following extensive interventions, including mechanical ventilation to manage severe symptoms, along with complications such as pneumothorax and a cardiac arrest episode, the infant exhibited a positive response to subsequent treatments. The infant responded positively to high-frequency oscillatory ventilation and inhaled nitric oxide. Gradual weaning from advanced ventilation led to successful extubation, followed by recovery with high-flow nasal cannula therapy. The case highlights the challenges of managing severe RSV infections in preterm infants and the efficacy of intensive care interventions in facilitating the infant's remarkable recovery and discharge.
Keywords: acute bronchiolitis; high flow nasal cannula (hfnc); high-frequency oscillator ventilator (hfov); inhaled nitric oxide; non-invasive positive pressure ventilation (nippv); pediatric intensive care unit(picu); positive end-expiratory pressure (peep); pressure control ventilation method; respiratory syncytial virus (rsv); respiratory tract.
Copyright © 2024, Alshihabi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Burden of respiratory syncytial virus bronchiolitis on the Dutch pediatric intensive care units.Eur J Pediatr. 2021 Oct;180(10):3141-3149. doi: 10.1007/s00431-021-04079-y. Epub 2021 Apr 23. Eur J Pediatr. 2021. PMID: 33891158 Free PMC article.
-
Effectiveness of Nasal Continuous Positive Airway Pressure vs Nasal Intermittent Positive Pressure Ventilation vs Noninvasive High-Frequency Oscillatory Ventilation as Support After Extubation of Neonates Born Extremely Preterm or With More Severe Respiratory Failure: A Secondary Analysis of a Randomized Clinical Trial.JAMA Netw Open. 2023 Jul 3;6(7):e2321644. doi: 10.1001/jamanetworkopen.2023.21644. JAMA Netw Open. 2023. PMID: 37399009 Free PMC article. Clinical Trial.
-
[High frequency oscillatory ventilation and conventional mechanical ventilation in the treatment of infants with severe respiratory syncytial virus pneumonia: a randomized controlled trial].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Apr;33(4):455-459. doi: 10.3760/cma.j.cn121430-20201106-00706. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 34053490 Clinical Trial. Chinese.
-
The infant with severe bronchiolitis: from high flow nasal cannula to continuous positive airway pressure and mechanical ventilation.Minerva Pediatr. 2018 Dec;70(6):612-622. doi: 10.23736/S0026-4946.18.05358-6. Epub 2018 Oct 18. Minerva Pediatr. 2018. PMID: 30334625 Review.
-
Children born preterm admitted to paediatric intensive care for bronchiolitis: a systematic review and meta-analysis.BMC Pediatr. 2023 Jun 29;23(1):326. doi: 10.1186/s12887-023-04150-7. BMC Pediatr. 2023. PMID: 37386478 Free PMC article.
References
-
- Severe RSV disease in preterm infants born at 29 to 35 weeks’ gestation in the United States. Ambrose CS. Pediatrics. 2014;134:1781. - PubMed
-
- Increased risk for respiratory syncytial virus-associated, community-acquired alveolar pneumonia in infants born at 31-36 weeks of gestation. Greenberg D, Dagan R, Shany E, Bar-Ziv J, Givon-Lavi N. Pediatr Infect Dis J. 2014;33:381–386. - PubMed
-
- Mechanical ventilatory support in infants with respiratory syncytial virus infection. Leclerc F, Scalfaro P, Noizet O, Thumerelle C, Dorkenoo A, Fourier C. Pediatr Crit Care Med. 2001;2:197–204. - PubMed
-
- Treatment of respiratory failure with inhaled nitric oxide and high- frequency ventilation in an infant with respiratory syncytial virus pneumonia and bronchopulmonary dysplasia. Hoehn T, Krause M, Krueger M, Hentschel R. Respiration. 1998;65:477–480. - PubMed
Publication types
LinkOut - more resources
Full Text Sources