

Genetic and clinical characterization of familial renal glucosuria
- PMID: 38344682
- PMCID: PMC10853784
- DOI: 10.1093/ckj/sfad265
Genetic and clinical characterization of familial renal glucosuria
Abstract
Background: Familial renal glucosuria (FRG) is a hereditary disorder caused by variants in SLC5A2 encoding sodium-glucose cotransporter 2 (SGLT2). In this study, we aimed to characterize proximal tubule solute transport, glucagon secretion and the genotype-phenotype relationship in FRG patients.
Methods: We sequenced SLC5A2 and PDZK1IP1 in 21 FRG patients and measured the renal threshold of glucose (RTG) in 15 patients. We built an open-source online calculator of RTG, evaluated the proximal tubule transport of amino acid, uric acid and phosphate, and explored glucagon secretion after glucose ingestion in FRG patients.
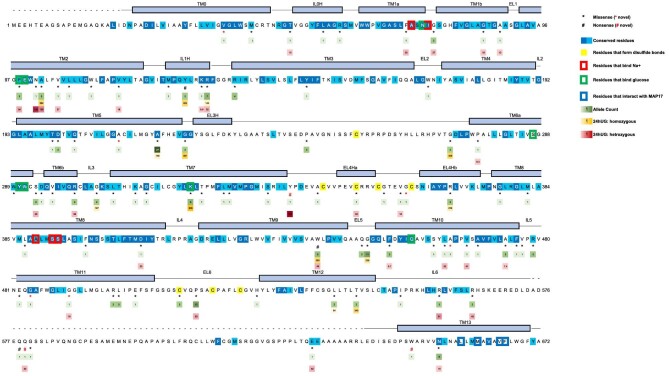
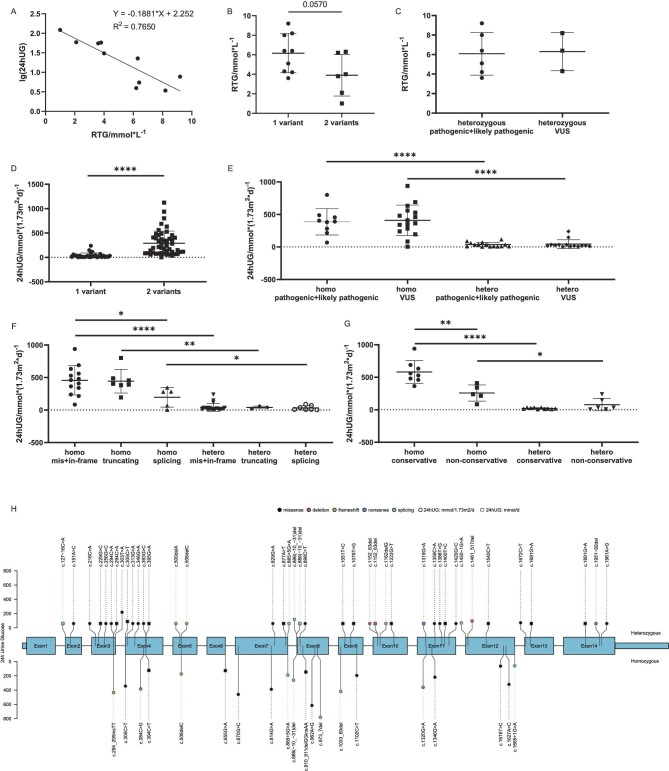
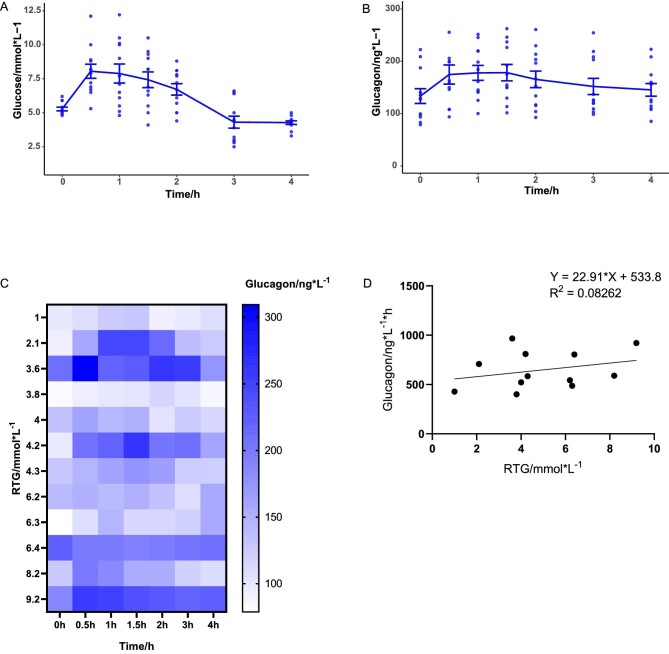
Results: We identified 12 novel SLC5A2 variants (G484D, R564W, A212S, c.574+1G>C, W649*, S592Cfs*6, Q579*, Y339*, V39F, G491E, A464E and G360D) in our cohort and yielded 111 SLC5A2 variants from literature review. RTG in our cohort ranged from 1.0 to 9.2 mmol/L. Patients with two SLC5A2 variants had lower RTG (3.9 vs 6.2 mmol/L) and higher 24-h urinary glucose excretion (24hUG) than single-variant carriers (291.0 vs 40.0 mmol/1.73 m2). Patients with homozygous missense or in-frame indels had mean 24hUG of 457.2 mmol/1.73 m2, comparable to those with homozygous truncating variants (445.0 mmol/1.73 m2) and significantly more than those with homozygous splicing variants (196.6 mmol/1.73 m2). Patients with homozygous missense variants involving conservative residues (582.0 mmol/1.73 m2) had more 24hUG than those with variants at non-conservative residues (257.6 mmol/1.73 m2). Four out of 14 tested patients had mild aminoaciduria. The RTG of FRG patients had no significant correlation to phosphate reabsorption but a potential negative correlation to the fractional excretion of uric acid. Postprandial suppression of glucagon secretion was absent in most FRG patients.
Conclusions: We built a comprehensive map showing the impact of SLC5A2 variant type and variant location on glucosuria severity. Our results highlighted the role of key residues in maintaining the transport function of SGLT2 and the functional link between glucosuria and reabsorption of amino acid and uric acid in FRG patients.
Keywords: SGLT2; SLC5A2; familial renal glucosuria; genotype–phenotype relationship.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures


References
LinkOut - more resources
Full Text Sources
