

Kidney Diseases Associated With Inflammatory Bowel Disease: Impact of Chronic Histologic Damage, Treatments, and Outcomes
- PMID: 38344742
- PMCID: PMC10851004
- DOI: 10.1016/j.ekir.2023.11.011
Kidney Diseases Associated With Inflammatory Bowel Disease: Impact of Chronic Histologic Damage, Treatments, and Outcomes
Abstract
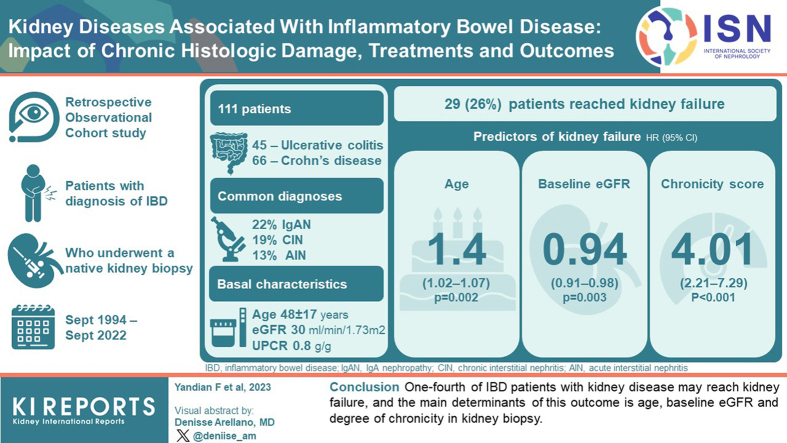
Introduction: Kidney disease is a well-known extraintestinal manifestation (EIM) associated with inflammatory bowel disease (IBD), with a variety of underlying etiologies. However, little is known about the overall outcomes and predictors.
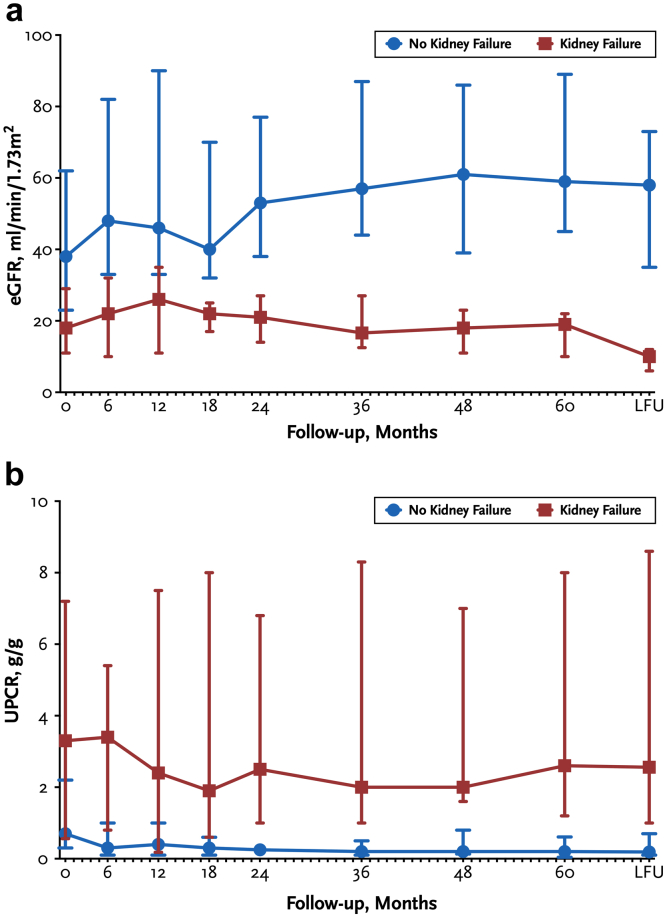
Methods: This is a retrospective, observational cohort study. Patients with IBD in whom a native kidney biopsy was performed at Mayo Clinic (Rochester, MN) between 1994 and 2022, were included. Demographic, clinical, and histologic characteristics of prognostic interest were collected. The main outcomes were kidney failure, disease remission, kidney function changes at last follow-up, and death.
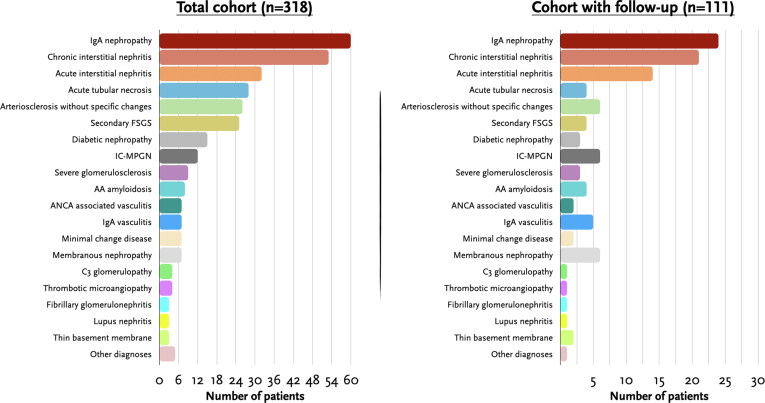
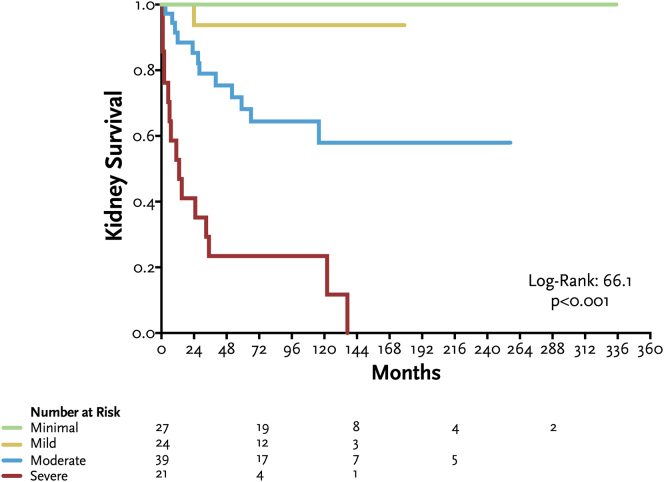
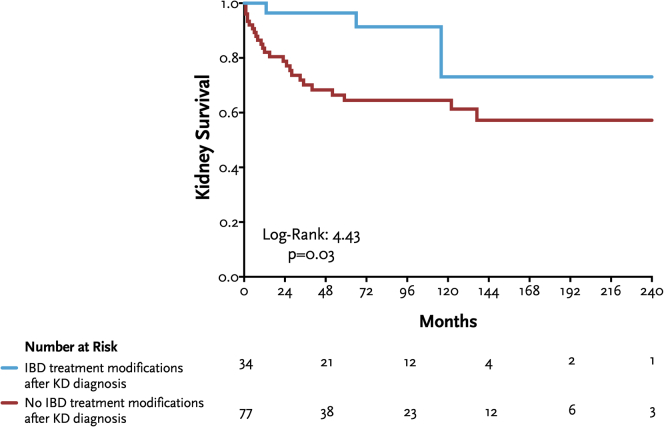
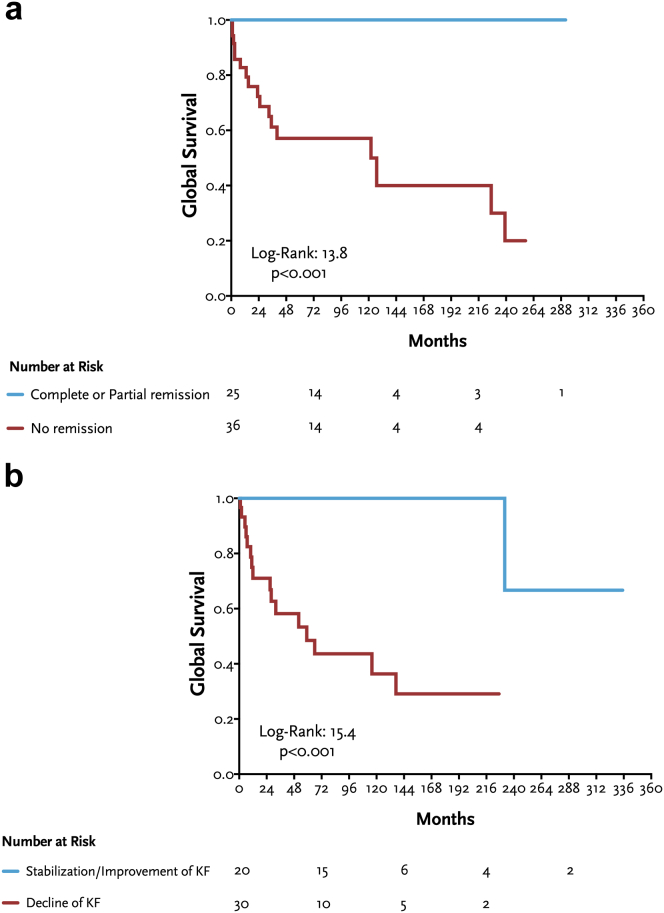
Results: From a total cohort of 318 patients, we selected a study group of 111 patients followed-up with at our institution (45 ulcerative colitis [UC] and 66 Crohn's disease [CD]), with a mean age of 48 ± 17 years (40% females). IgA nephropathy (IgAN), chronic interstitial nephritis (CIN), and acute interstitial nephritis (AIN) were the most common diagnoses (22%, 19%, 13%, respectively). Median estimated glomerular filtration rate (eGFR) at presentation was 30 ml/min per 1.73 m2 (interquartile range [IQR]: 17-54) and urinary protein-to-creatinine ratio [UPCR] 0.8 g/g (0.3-3.4), without differences between IBD types. During a median follow-up of 59 months (12-109), 29 patients (26%) reached kidney failure. By multivariable analysis, the main predictors of kidney failure were age (hazard ratio [HR]: 1.04; P = 0.002), baseline eGFR (HR: 0.94; P = 0.003) and histologic chronicity score (HR: 4.01; P < 0.001). Therapeutic management varied according to underlying etiology. Global survival (kidney failure + death) was significantly better in patients who achieved complete or partial remission, or stabilization or improvement of kidney function.
Conclusion: One-fourth of patients with IBD with kidney disease may reach kidney failure, and the main determinants of this outcome is age, baseline eGFR, and degree of chronicity in kidney biopsy.
Keywords: IgA nephropathy; inflammatory bowel disease; interstitial nephritis; kidney failure; total chronicity score.
© 2023 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
