

SF-CORNER (splenic flexure colorectal cancer): an international survey of operative approaches and outcomes for cancers of the splenic flexure
- PMID: 38345176
- PMCID: PMC12150829
- DOI: 10.1111/codi.16895
SF-CORNER (splenic flexure colorectal cancer): an international survey of operative approaches and outcomes for cancers of the splenic flexure
Abstract
Aim: The optimum surgical approach to splenic flexure cancers (SFCs) remains uncertain. The aim of this survey was to explore the opinions of an international surgical community on the management and outcomes of SFC.
Method: A questionnaire was constructed comprising five sections (information about respondents; definition and prognosis of SFC; operative approach; approach in specific scenarios; outcomes) and circulated through an international dissemination committee and social media.
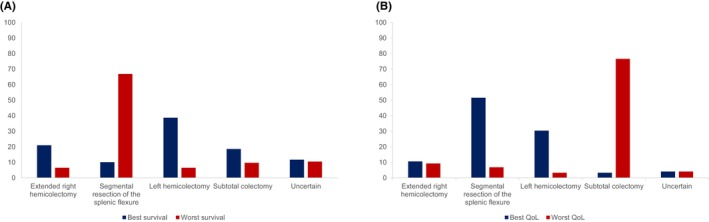
Results: The survey received 576 responses over 4 weeks across 50 countries. There was no consensus regarding the definition of the splenic flexure, whilst the proportion of respondents who did and did not think that patients with SFC had a worse outcome was equal. The overall preferred operative approach was left hemicolectomy [203 (35.2%)], followed by segmental resection [167 (29%)], extended right hemicolectomy [126 (21.9%)] and subtotal colectomy [7 (12%)]. The stated pedicles for ligation varied between resection types and also within the same resection. One hundred and sixty-six (28.8%) respondents thought a segmental resection was associated with the worst survival and 190 (33%) thought it was associated with the best quality of life.
Conclusion: This survey confirms a lack of consensus across all aspects SFC treatment. The differing approaches described are likely to represent different beliefs around the variable anatomy of this region and the associated lymphatic drainage. Future studies are required to address such inconsistencies and identify the optimum surgical strategy, whilst also incorporating quality-of-life metrics and patient-reported outcomes. A one-size-fits-all approach is probably not appropriate with SFC, and a more bespoke approach is required.
Keywords: colonic resection; nodal mapping; personalised treatment; splenic flexure cancers.
© 2024 The Authors. Colorectal Disease published by John Wiley & Sons Ltd on behalf of Association of Coloproctology of Great Britain and Ireland.
Conflict of interest statement
All authors have no conflicts of interest to declare.
Figures

References
-
- Binda GA, Amato A, Alberton G, Bruzzone M, Secondo P, Lòpez‐Borao J, et al. Surgical treatment of a colon neoplasm of the splenic flexure: a multicentric study of short‐term outcomes. Colorectal Dis. 2020;22(2):146–153. - PubMed
-
- de'Angelis N, Martínez‐Pérez A, Winter DC, Landi F, Vitali GC, Le Roy B, et al. Extended right colectomy, left colectomy, or segmental left colectomy for splenic flexure carcinomas: a European multicenter propensity score matching analysis. Surg Endosc. 2021;35(2):661–672. - PubMed
-
- Martín Arévalo J, Moro‐Valdezate D, García‐Botello SA, Pla‐Martí V, Garcés‐Albir M, Pérez Santiago L, et al. Propensity score analysis of postoperative and oncological outcomes after surgical treatment for splenic flexure colon cancer. Int J Colorectal Dis. 2018;33(9):1201–1213. - PubMed
-
- Nakagoe T, Sawai T, Tsuji T, Jibiki M, Ohbatake M, Nanashima A, et al. Surgical treatment and subsequent outcome of patients with carcinoma of the splenic flexure. Surg Today. 2001;31(3):204–209. - PubMed
-
- Odermatt M, Siddiqi N, Johns R, Miskovic D, Khan O, Khan J, et al. Short‐ and long‐term outcomes for patients with splenic flexure tumours treated by left versus extended right colectomy are comparable: a retrospective analysis. Surg Today. 2014;44(11):2045–2051. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
