

Comprehensive temporal analysis of right ventricular function and pulmonary haemodynamics in mechanically ventilated COVID-19 ARDS patients
- PMID: 38345712
- PMCID: PMC10861421
- DOI: 10.1186/s13613-024-01241-1
Comprehensive temporal analysis of right ventricular function and pulmonary haemodynamics in mechanically ventilated COVID-19 ARDS patients
Abstract
Background: Cardiac injury is frequently reported in COVID-19 patients, the right ventricle (RV) is mostly affected. We systematically evaluated the cardiac function and longitudinal changes in severe COVID-19 acute respiratory distress syndrome (ARDS) admitted to the intensive care unit (ICU) and assessed the impact on survival.
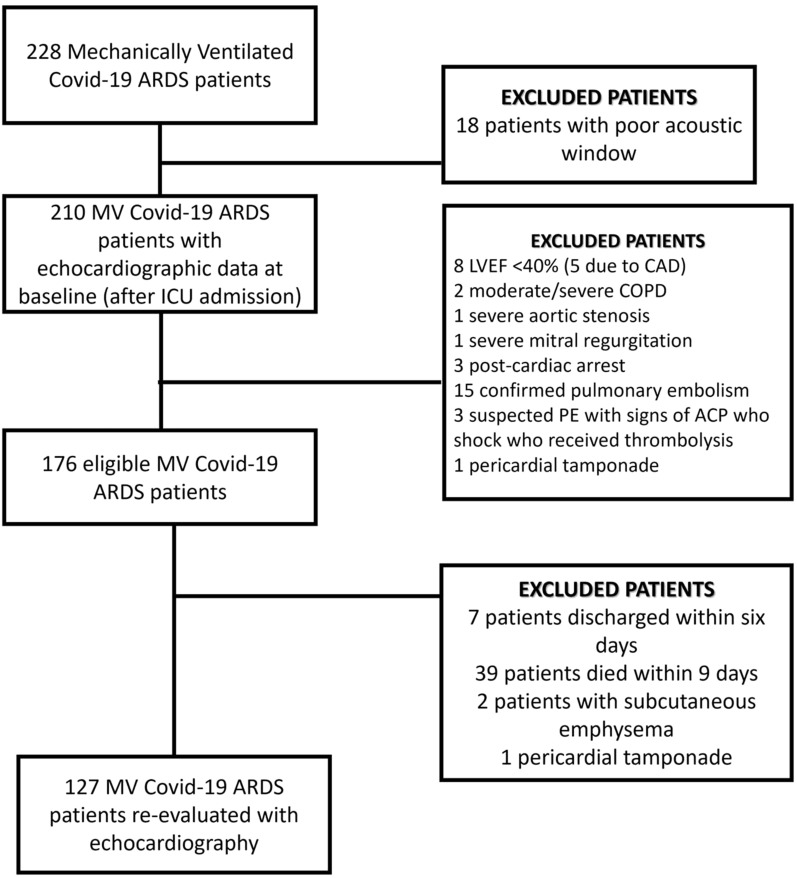
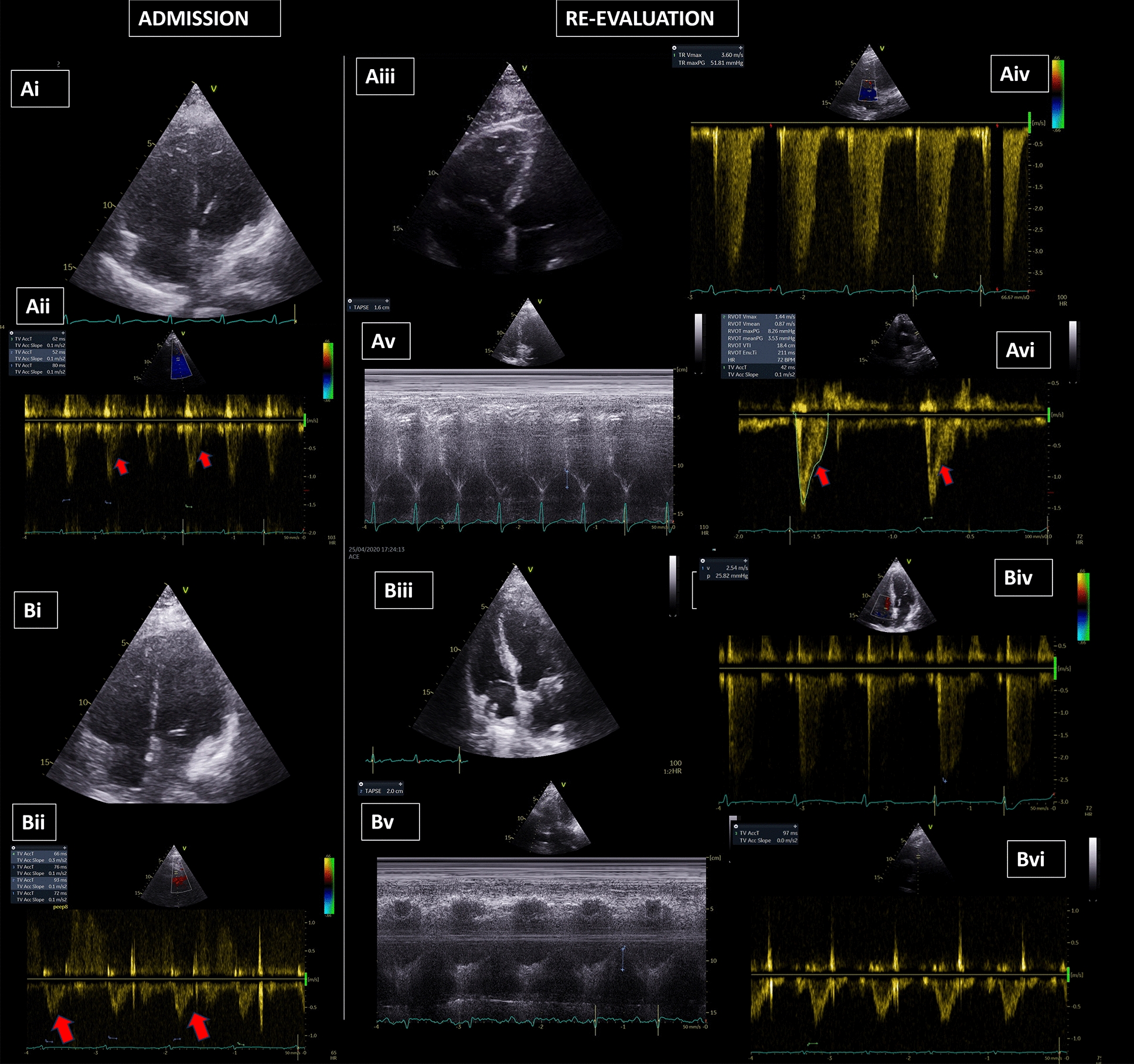
Methods: We prospectively performed comprehensive echocardiographic analysis on mechanically ventilated COVID-19 ARDS patients, using 2D/3D echocardiography. We defined left ventricular (LV) systolic dysfunction as ejection fraction (EF) < 40%, or longitudinal strain (LS) > - 18% and right ventricular (RV) dysfunction if two indices among fractional area change (FAC) < 35%, tricuspid annulus systolic plane excursion (TAPSE) < 1.6 cm, RV EF < 44%, RV-LS > - 20% were present. RV afterload was assessed from pulmonary artery systolic pressure (PASP), PASP/Velocity Time Integral in the right ventricular outflow tract (VTIRVOT) and pulmonary acceleration time (PAcT). TAPSE/PASP assessed the right ventriculoarterial coupling (VACR).
Results: Among 176 patients included, RV dysfunction was common (69%) (RV-EF 41.1 ± 1.3%; RV-FAC 36.6 ± 0.9%, TAPSE 20.4 ± 0.4mm, RV-LS:- 14.4 ± 0.4%), usually accompanied by RV dilatation (RVEDA/LVEDA 0.82 ± 0.02). RV afterload was increased in most of the patients (PASP 33 ± 1.1 mmHg, PAcT 65.3 ± 1.5 ms, PASP/VTIRVOT, 2.29 ± 0.1 mmHg/cm). VACR was 0.8 ± 0.06 mm/mmHg. LV-EF < 40% was present in 21/176 (11.9%); mean LV-EF 57.8 ± 1.1%. LV-LS (- 13.3 ± 0.3%) revealed a silent LV impairment in 87.5%. A mild pericardial effusion was present in 70(38%) patients, more frequently in non-survivors (p < 0.05). Survivors presented significant improvements in respiratory physiology during the 10th ICU-day (PaO2/FiO2, 231.2 ± 11.9 vs 120.2 ± 6.7 mmHg; PaCO2, 43.1 ± 1.2 vs 53.9 ± 1.5 mmHg; respiratory system compliance-CRS, 42.6 ± 2.2 vs 27.8 ± 0.9 ml/cmH2O, all p < 0.0001). Moreover, survivors presented significant decreases in RV afterload (PASP: 36.1 ± 2.4 to 20.1 ± 3 mmHg, p < 0.0001, PASP/VTIRVOT: 2.5 ± 1.4 to 1.1 ± 0.7, p < 0.0001 PAcT: 61 ± 2.5 to 84.7 ± 2.4 ms, p < 0.0001), associated with RV systolic function improvement (RVEF: 36.5 ± 2.9% to 46.6 ± 2.1%, p = 0.001 and RV-LS: - 13.6 ± 0.7% to - 16.7 ± 0.8%, p = 0.001). In addition, RV dilation subsided in survivors (RVEDA/LVEDA: 0.8 ± 0.05 to 0.6 ± 0.03, p = 0.001). Day-10 CRS correlated with RV afterload (PASP/VTIRVOT, r: 0.535, p < 0.0001) and systolic function (RV-LS, 0.345, p = 0.001). LV-LS during the 10th ICU-day, while ΔRV-LS and ΔPASP/RVOTVTI were associated with survival.
Conclusions: COVID-19 improvements in RV function, RV afterload and RV-PA coupling at day 10 were associated with respiratory function and survival.
Keywords: ARDS; COVID-19; Cardiac function; Hemodynamics; PEEP; Pulmonary vascular resistance; RV dysfunction; Strain.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests related to the present study.
Figures
References
-
- Task Force for The Management of COVID-19 of The European Society of Cardiology European Society of Cardiology guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: part 1-epidemiology, pathophysiology, and diagnosis. Eur Heart J. 2021 doi: 10.1093/eurheartj/ehab696. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
