

Rotavirus and adenovirus infections in children with acute gastroenteritis after introducing the Rotasiil® vaccine in Kisangani, Democratic Republic of the Congo
- PMID: 38346035
- PMCID: PMC10861064
- DOI: 10.1371/journal.pone.0297219
Rotavirus and adenovirus infections in children with acute gastroenteritis after introducing the Rotasiil® vaccine in Kisangani, Democratic Republic of the Congo
Abstract
Background: Although rotavirus vaccination has reduced the global burden of the virus, morbidity and mortality from rotavirus infection remain high in Sub-Saharan Africa. This study aimed to determine the prevalence of rotavirus and adenovirus infections in children under five years with acute gastroenteritis and to identify factors associated with rotavirus infection after the introduction of the Rotasiil® vaccine in 2019 in Kisangani, Democratic Republic of the Congo (DRC).
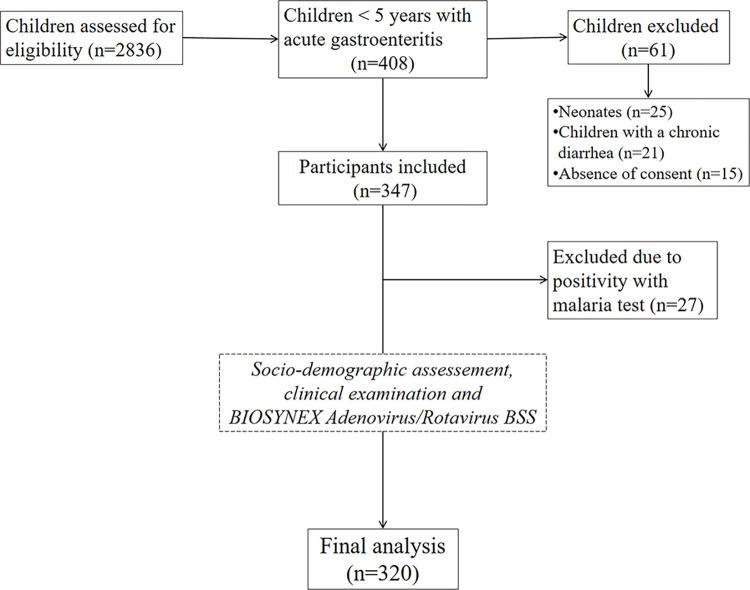
Methods: This study consisted of a cross-sectional hospital-based survey conducted from May 2022 to April 2023 in four health facilities in Kisangani, using a fecal-based test (rapid antigenic immuno-chromatographic diagnostic test, BYOSYNEX adenovirus/rotavirus BSS, Biosynex SA, Illkirch-Graffenstaden, France) of rotavirus and adenovirus infections among children under five years of age with acute gastroenteritis.
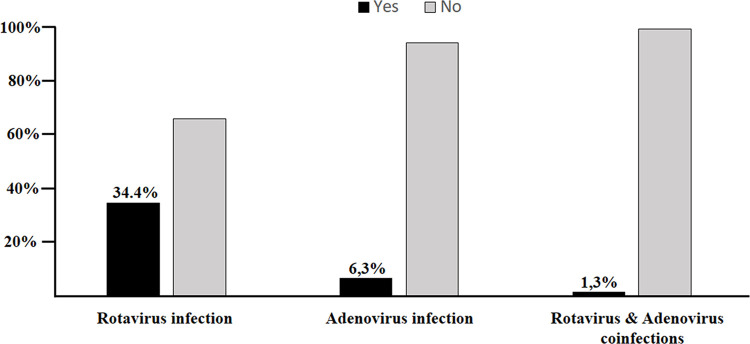
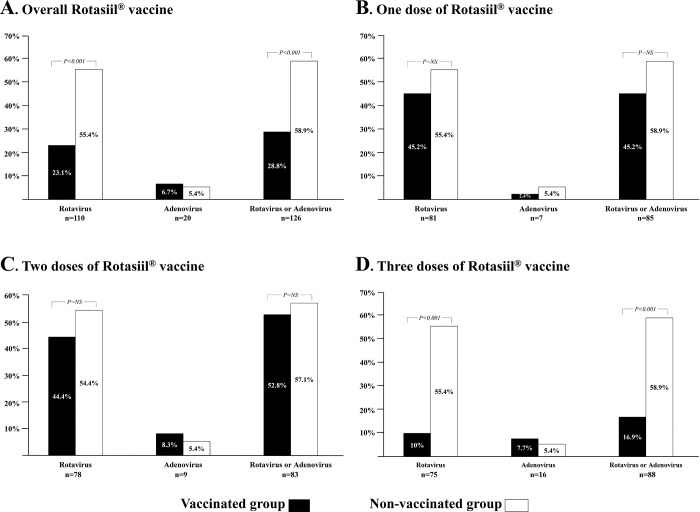
Results: A total of 320 children under five years of age with acute gastroenteritis were included. The prevalence of rotavirus infection was 34.4%, that of adenovirus was 6.3%, and that of both rotavirus and adenovirus coinfection was 1.3%. The prevalence of rotavirus was significantly higher in unvaccinated children than in vaccinated children (55.4% versus 23.1%; P < 0.001). This difference was observed only in children who received all three vaccine doses. Multivariate logistic regression analysis shows that the rate of rotavirus infection was significantly reduced in vaccinated children (adjusted OR: 0.31 [95% confidence intervals (CI): 0.19-0.56]; P < 0.001) and those whose mothers had an average (adjusted OR: 0.51 [95% CI: 0.25-0.91]; P = 0.018) or high level (adjusted OR: 0.34 [95% CI: 0.20-0.64]; P < 0.001) of knowledge about the rotavirus vaccine.
Conclusions: The prevalence of rotavirus infection remains high in Kisangani despite vaccination. However, the prevalence of adenovirus infections was low in our series. Complete vaccination with three doses and mothers' average and high level of knowledge about the rotavirus vaccine significantly reduces the rate of rotavirus infection. It is, therefore, essential to strengthen the mothers' health education, continue with the Rotasiil® vaccine, and ensure epidemiological surveillance of rotavirus infection.
Copyright: © 2024 Manzemu et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Clinical profile of children under 5 years of age with rotavirus diarrhoea in a hospital setting in Kisangani, DRC, after the introduction of the rotavirus vaccine, a cross-sectional study.BMC Pediatr. 2023 Apr 24;23(1):193. doi: 10.1186/s12887-023-04022-0. BMC Pediatr. 2023. PMID: 37095482 Free PMC article.
-
Molecular epidemiology and surveillance of circulating rotavirus and adenovirus in Congolese children with gastroenteritis.J Med Virol. 2016 Apr;88(4):596-605. doi: 10.1002/jmv.24382. Epub 2015 Sep 28. J Med Virol. 2016. PMID: 26378607
-
Epidemiology and pre-vaccine burden of rotavirus diarrhea in Democratic Republic of Congo (DRC): Results of sentinel surveillance, 2009-2019.Vaccine. 2022 Sep 29;40(41):5933-5941. doi: 10.1016/j.vaccine.2022.08.041. Epub 2022 Sep 6. Vaccine. 2022. PMID: 36068112 Free PMC article.
-
Population effectiveness of the pentavalent and monovalent rotavirus vaccines: a systematic review and meta-analysis of observational studies.BMC Infect Dis. 2017 Aug 15;17(1):569. doi: 10.1186/s12879-017-2613-4. BMC Infect Dis. 2017. PMID: 28810833 Free PMC article.
-
Association of Rotavirus Vaccines With Reduction in Rotavirus Gastroenteritis in Children Younger Than 5 Years: A Systematic Review and Meta-analysis of Randomized Clinical Trials and Observational Studies.JAMA Pediatr. 2021 Jul 1;175(7):e210347. doi: 10.1001/jamapediatrics.2021.0347. Epub 2021 Jul 6. JAMA Pediatr. 2021. PMID: 33970192 Free PMC article.
Cited by
-
Driving forces of continuing evolution of rotaviruses.World J Virol. 2024 Jun 25;13(2):93774. doi: 10.5501/wjv.v13.i2.93774. World J Virol. 2024. PMID: 38984077 Free PMC article. Review.
-
The prevalence of rotavirus infection among Congolese children younger than 5 years hospitalized for gastroenteritis 10 years after introduction of rotavirus vaccination.IJID Reg. 2025 Feb 13;14:100596. doi: 10.1016/j.ijregi.2025.100596. eCollection 2025 Mar. IJID Reg. 2025. PMID: 40144537 Free PMC article.
References
-
- Qazi S, Aboubaker S, MacLean R, Fontaine O, Mantel C, Goodman T, et al.. Ending preventable child deaths from pneumonia and diarrhoea by 2025. Development of the integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea. Arch Dis Child. 2015. Feb;100 Suppl 1:S23–8. doi: 10.1136/archdischild-2013-305429 - DOI - PubMed
-
- World Health Organization (WHO). Weekly epidemiological record. Rotavirus vaccines: WHOposition paper. Available from https://apps.who.int/iris/bitstream/handle/10665/342904/WER9628-eng-fre.pdf Accessed August 19, 2023
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
