

Infiltration of CD3+ and CD8+ lymphocytes in association with inflammation and survival in pancreatic cancer
- PMID: 38346068
- PMCID: PMC10861089
- DOI: 10.1371/journal.pone.0297325
Infiltration of CD3+ and CD8+ lymphocytes in association with inflammation and survival in pancreatic cancer
Abstract
Background: Pancreatic ductal adenocarcinomas (PDAC) have heterogeneous tumor microenvironments relatively devoid of infiltrating immune cells. We aimed to quantitatively assess infiltrating CD3+ and CD8+ lymphocytes in a treatment-naïve patient cohort and assess associations with overall survival and microenvironment inflammatory proteins.
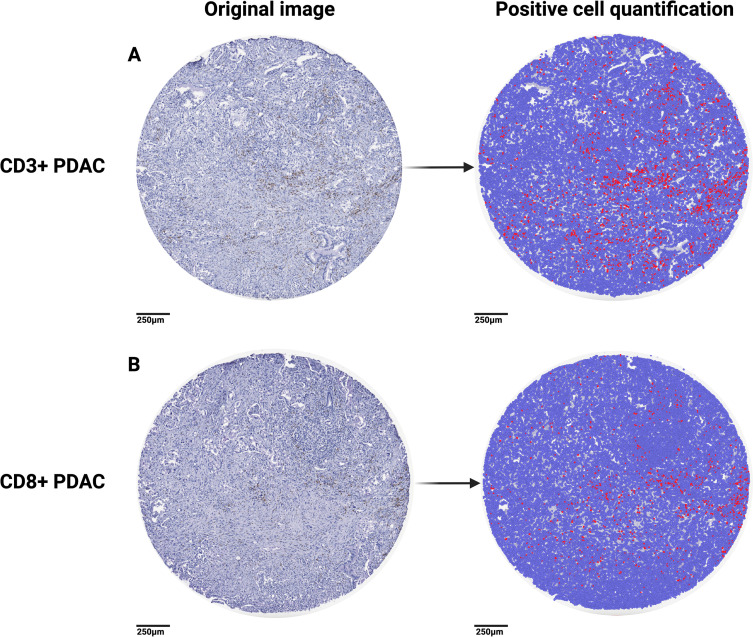
Methods: Tissue microarrays were immunohistochemically stained for CD3+ and CD8+ lymphocytes and quantitatively assessed using QuPath. Levels of inflammation-associated proteins were quantified by multiplexed, enzyme-linked immunosorbent assay panels on matching tumor and tissue samples.
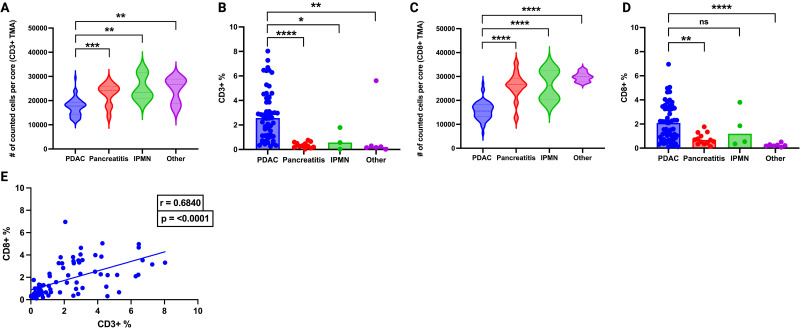
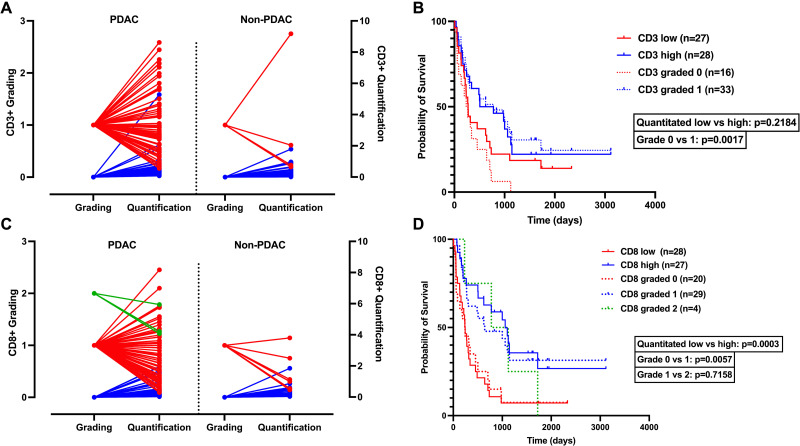
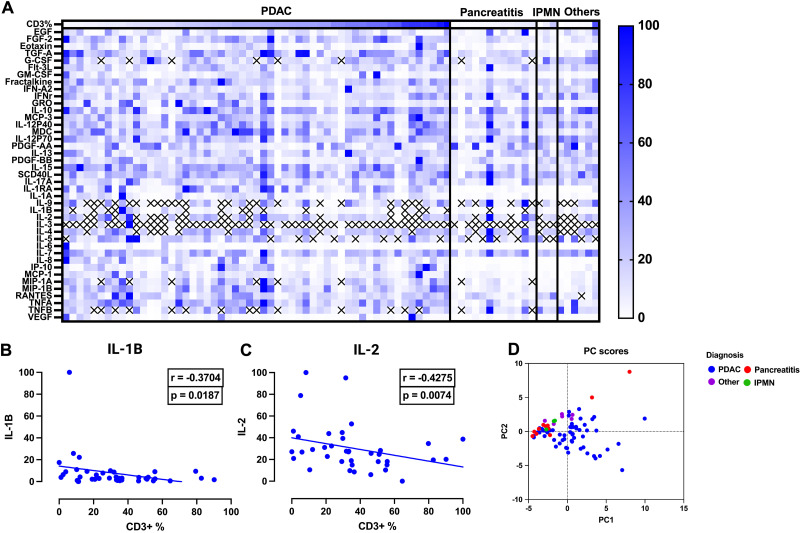
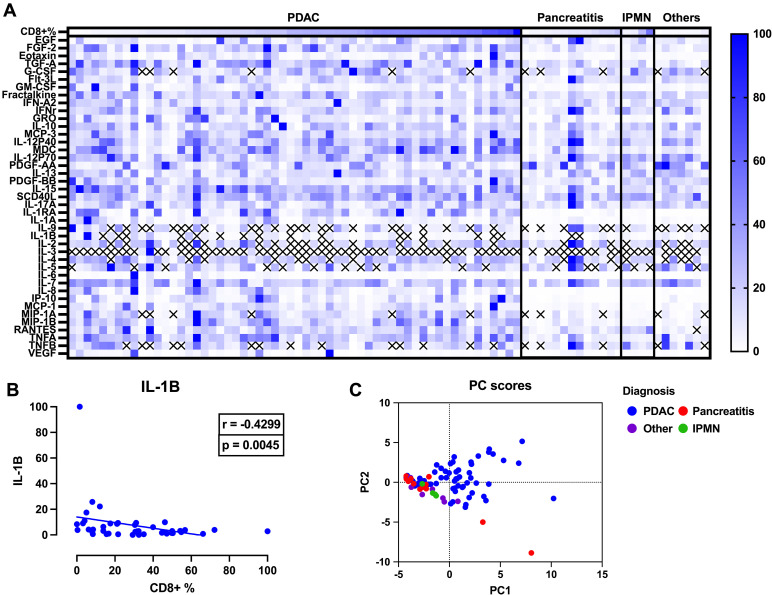
Results: Our findings revealed a significant increase in both CD3+ and CD8+ lymphocytes populations in PDAC compared with non-PDAC tissue, except when comparing CD8+ percentages in PDAC versus intraductal papillary mucinous neoplasms (IPMN) (p = 0.5012). Patients with quantitatively assessed CD3+ low tumors (lower 50%) had shorter survival (median 273 days) compared to CD3+ high tumors (upper 50%) with a median overall survival of 642.5 days (p = 0.2184). Patients with quantitatively assessed CD8+ low tumors had significantly shorter survival (median 240 days) compared to CD8+ high tumors with a median overall survival of 1059 days (p = 0.0003). Of 41 proteins assessed in the inflammation assay, higher levels of IL-1B and IL-2 were significantly associated with decreased CD3+ infiltration (r = -0.3704, p = 0.0187, and r = -0.4275, p = 0.0074, respectively). Higher levels of IL-1B were also significantly associated with decreased CD8+ infiltration (r = -0.4299, p = 0.0045), but not IL-2 (r = -0.0078, p = 0.9616). Principal component analysis of the inflammatory analytes showed diverse inflammatory responses in PDAC.
Conclusion: In this work, we found a marked heterogeneity in infiltrating CD3+ and CD8+ lymphocytes and individual inflammatory responses in PDAC. Future mechanistic studies should explore personalized therapeutic strategies to target the immune and inflammatory components of the tumor microenvironment.
Copyright: © 2024 Tushoski-Alemán et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
