

Efficacy of intraoperative systemic lidocaine on quality of recovery after laparoscopic colorectal surgery: a randomized controlled trial
- PMID: 38346397
- PMCID: PMC10863528
- DOI: 10.1080/07853890.2024.2315229
Efficacy of intraoperative systemic lidocaine on quality of recovery after laparoscopic colorectal surgery: a randomized controlled trial
Abstract
Introduction: Many clinical trials have demonstrated the benefits of intraoperative systemic lidocaine administration in major abdominal surgeries. We tested the hypothesis that systemic lidocaine is associated with an enhanced early quality of recovery in patients following laparoscopic colorectal resection.
Patients and methods: We randomly allocated 126 patients scheduled for laparoscopic colorectal surgery in a 1:1 ratio to receive either lidocaine (1.5 mg kg-1 bolus over 10 min, followed by continuous infusion at 2 mg kg-1 h-1 until the end of surgery) or identical volumes and rates of saline. The primary outcome was the Quality of Recovery-15 score assessed 24 h after surgery. Secondary outcomes were areas under the pain numeric rating scale curve over time, 48-h morphine consumption, and adverse events.
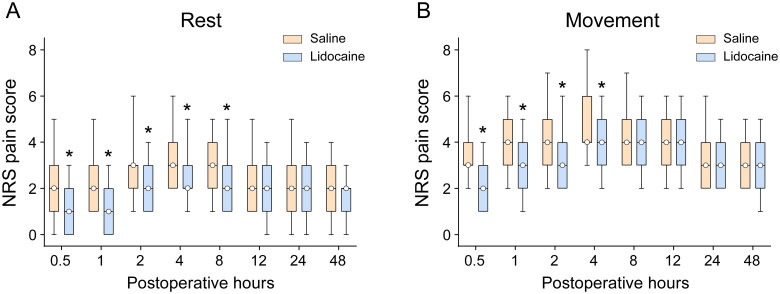
Results: Compared with saline, systemic lidocaine improved the Quality of Recovery-15 score 24 h postoperatively, with a median difference of 4 (95% confidence interval: 1-6; p = 0.015). Similarly, the area under the pain numeric rating scale curve over 48 h at rest and on movement was reduced in the lidocaine group (p = 0.004 and p < 0.001, respectively). However, these differences were not clinically meaningful. Lidocaine infusion reduced the intraoperative remifentanil requirements but not postoperative 48-h morphine consumption (p < 0.001 and p = 0.34, respectively). Additionally, patients receiving lidocaine had a quicker and earlier return of bowel function, as indicated by a shorter time to first flatus (log-rank p < 0.001), yet ambulation time was similar between groups (log-rank test, p = 0.11).
Conclusions: In patients undergoing laparoscopic colorectal surgery, intraoperative systemic lidocaine resulted in statistically but not clinically significant improvements in quality of recovery (see Graphical Abstract).Trial registration: Chinese Clinical Trial Registry; ChiCTR1900027635.
Keywords: Colorectal surgery; lidocaine; pain management; post-surgical recovery.
Plain language summary
Systemic lidocaine failed to clinically improve the overall quality of recovery following laparoscopic colorectal resection.Systemic lidocaine reduced intraoperative remifentanil and time to first flatus but not postoperative 48-h morphine consumption.No differences emerged in patient-reported outcomes like opioid side effects, mobility, or satisfaction between groups postoperatively.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures




References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources