

An Unusual Abscess Associated with Gallbladder Perforation Successfully Treated with Percutaneous Transhepatic Gallbladder Drainage and Endoscopic Ultrasound-guided Abscess Drainage
- PMID: 38346739
- PMCID: PMC11473268
- DOI: 10.2169/internalmedicine.2963-23
An Unusual Abscess Associated with Gallbladder Perforation Successfully Treated with Percutaneous Transhepatic Gallbladder Drainage and Endoscopic Ultrasound-guided Abscess Drainage
Abstract
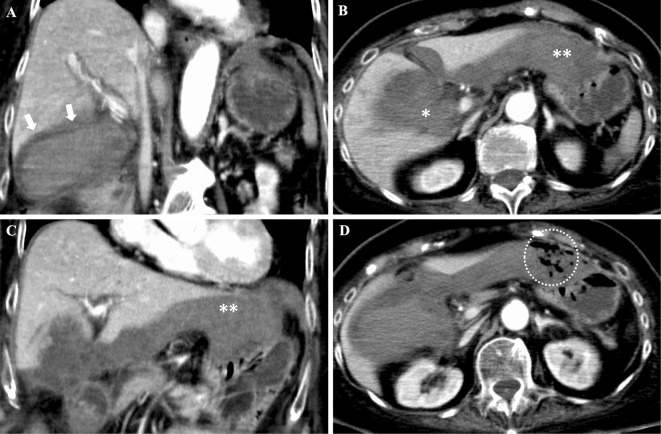
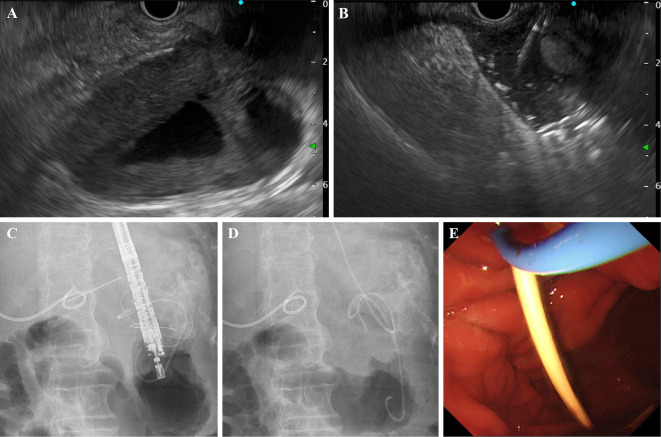
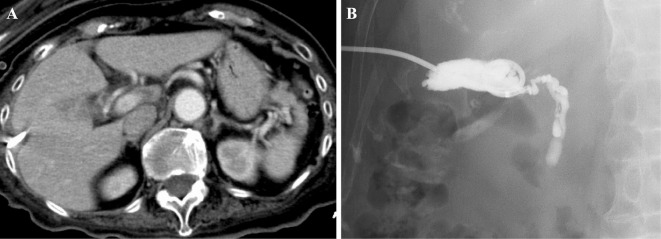
Abscesses associated with gallbladder perforation are often confined to the peri-gallbladder region. We herein report a rare case of gallbladder perforation in which the abscess cavity extended into the left upper quadrant. A 79-year-old woman developed gallbladder perforation secondary to acalculous cholecystitis. Computed tomography revealed fluid collection extending from the peri-gallbladder to the dorsal left hepatic lobe in contact with the stomach. We successfully treated percutaneous transhepatic gallbladder drainage and simultaneous endoscopic ultrasound-guided transgastric internal and external abscess drainage. This minimally invasive approach is considered safe and feasible for managing such a rare case.
Keywords: EUS; abscess; drainage; gallbladder perforation; interventional EUS.
Conflict of interest statement
Figures

References
-
- Stefanidis D, Sirinek KR, Bingener J. Gallbladder perforation: risk factors and outcome. J Surg Res 131: 204-208, 2006. - PubMed
-
- Weiss CA 3rd, Lakshman TV, Schwartz RW. Current diagnosis and treatment of cholecystitis. Curr Surg 59: 51-54, 2002. - PubMed
-
- Fry DE, Cox RA, Harbrecht PJ. Gangrene of the gallbladder: a complication of acute cholecystitis. South Med J 74: 666-668, 1981. - PubMed