

Influence of metabolic state and body composition on the action of pharmacological treatment of migraine
- PMID: 38347465
- PMCID: PMC10863119
- DOI: 10.1186/s10194-024-01724-3
Influence of metabolic state and body composition on the action of pharmacological treatment of migraine
Abstract
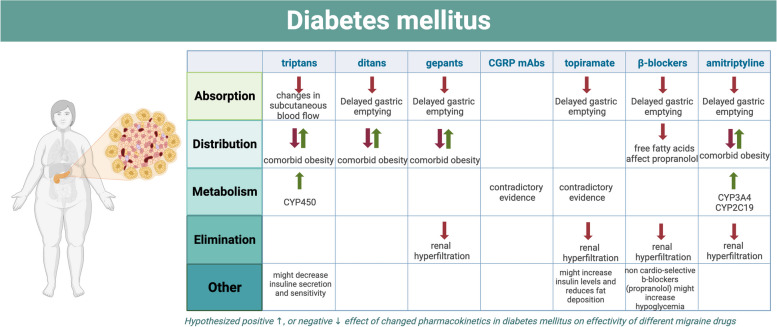
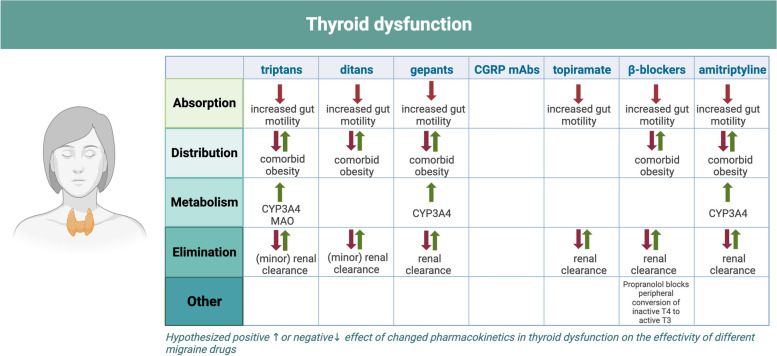
Migraine is a disabling neurovascular disorder among people of all ages, with the highest prevalence in the fertile years, and in women. Migraine impacts the quality of life of affected individuals tremendously and, in addition, it is associated with highly prevalent metabolic diseases, such as obesity, diabetes mellitus and thyroid dysfunction. Also, the clinical response to drugs might be affected in patients with metabolic disease due to body composition and metabolic change. Therefore, the efficacy of antimigraine drugs could be altered in patients with both migraine and metabolic disease. However, knowledge of the pharmacology and the related clinical effects of antimigraine drugs in patients with metabolic disease are limited. Therefore, and given the clinical relevance, this article provides a comprehensive overview of the current research and hypotheses related to the influence of metabolic state and body composition on the action of antimigraine drugs. In addition, the influence of antimigraine drugs on metabolic functioning and, vice versa, the influence of metabolic diseases and its hormonal modulating medication on migraine activity is outlined. Future exploration on personalizing migraine treatment to individual characteristics is necessary to enhance therapeutic strategies, especially given its increasing significance in recent decades.
Keywords: CGRP; Diabetes mellitus; Lifestyle; Metabolic disorders; Migraine; Obesity.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Olesen J (2018) Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Vol. 38, Cephalalgia. SAGE Publications Ltd; p. 1–211 - PubMed
-
- Stovner LJ, Nichols E, Steiner TJ, Abd-Allah F, Abdelalim A, Al-Raddadi RM, et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi: 10.1016/S1474-4422(18)30322-3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
