

Effects of surgical management for gastrointestinal stromal tumor patients with liver metastasis on survival outcomes
- PMID: 38347834
- PMCID: PMC10860711
- DOI: 10.3389/fonc.2024.1289885
Effects of surgical management for gastrointestinal stromal tumor patients with liver metastasis on survival outcomes
Abstract
Purpose: To investigate the effect of surgical resection on survival in gastrointestinal stromal tumors synchronous liver metastasis (GIST-SLM) and to develop clinically usable predictive models for overall survival (OS) and cancer-specific survival (CSS) in patients.
Methods: We identified patients in the SEER database diagnosed with GISTs from 2010 to 2019. We used propensity score matching (PSM) to balance the bias between the Surgery and No surgery groups. Kaplan-Meier(K-M) analysis was used to detect differences in OS and CSS between the two groups. The nomogram to predict 1, 3, and 5-year OS and CSS were developed and evaluated.
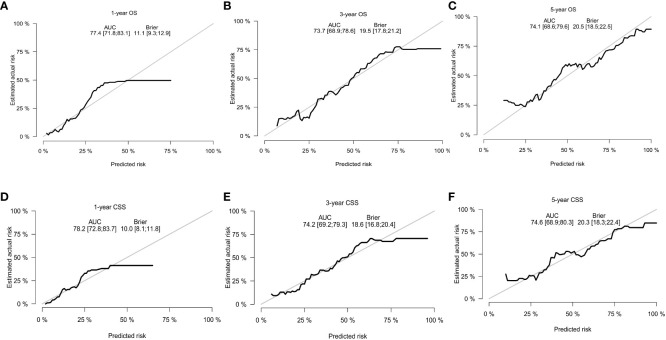
Results: After PSM, 228 patients were included in this study. There were significant differences in 1, 3, and 5-year OS and CSS between the two groups (OS: 93.5% vs. 84.4%, 73.2% vs. 55.3%, 60.9% vs. 36.9%, P=0.014; CSS: 3.5% vs.86.2%,75.3% vs.57.9%, 62.6% vs. 42.9%, P=0.02). We also found that patients who received surgery combined with targeted therapy had better OS and CSS at 1, 3, and 5 years than those who received surgery only (OS: 96.6% vs.90.9%, 74.9% vs. 56.8%, 61.7% vs. 35.5%, P=0.022; CSS: 96.6% vs. 92.1%, 77.4% vs.59.2%,63.8% vs. 42.0%, P=0.023). The area under the curve (AUC) was 0.774, 0.737, and 0.741 for 1, 3, and 5-year OS, respectively, with 0.782 and 0.742 for 1, 3, and 5-year CSS. In the model, C-index was 0.703 for OS and 0.705 for CSS and showed good consistency.
Conclusion: Surgical treatment can improve the OS and CSS of patients with GIST-SLM. In addition, the combination with chemotherapy may be more favorable for the long-term survival of patients. Meanwhile, we constructed the nomograms for predicting OS and CSS at 1, 3, and 5-year, and validated them internally. Our model can contribute to clinical management and treatment strategy optimization.
Keywords: gastrointestinal stromal tumor; nomograms; surgery; survival; synchronous liver metastasis.
Copyright © 2024 Liu, Xia, Ju, Zhang, Shi, Du, Zhan and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
LinkOut - more resources
Full Text Sources
Miscellaneous