

Distinct clinical characteristics in stage III rectal cancer among different age groups and treatment outcomes after neoadjuvant chemoradiotherapy
- PMID: 38347922
- PMCID: PMC10860489
- DOI: 10.1177/17588359241229434
Distinct clinical characteristics in stage III rectal cancer among different age groups and treatment outcomes after neoadjuvant chemoradiotherapy
Abstract
Background: There is a rapidly increasing incidence of early-onset colorectal cancer (EO-CRC) which threatens the survival of young people, while aging also represents a challenging clinical problem.
Objectives: We aimed to investigate the differences in the clinical characteristics and prognosis in stage III rectal cancer (RC), to help optimize treatment strategies.
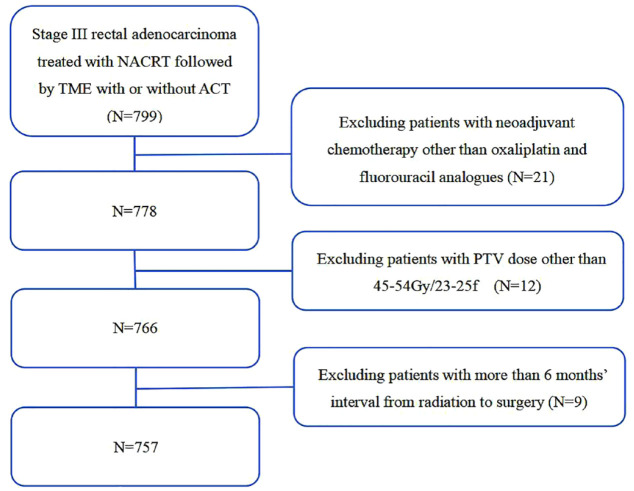
Design and methods: This study included 757 patients with stage III RC, all of whom received neoadjuvant chemoradiotherapy and total mesorectal excision. The whole cohort was categorized as very early onset (VEO, ⩽30 years old), early onset (EO, >30 years old, ⩽50 years old), intermediate onset (IO, >50 years, ⩽70 years), or late onset (LO, >70 years old).
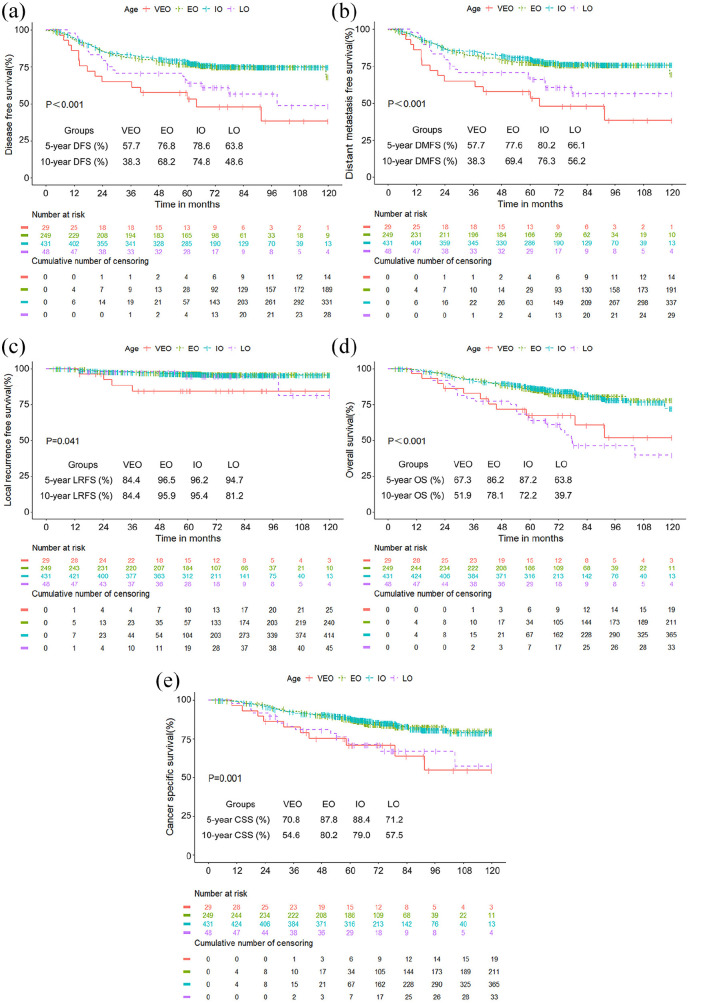
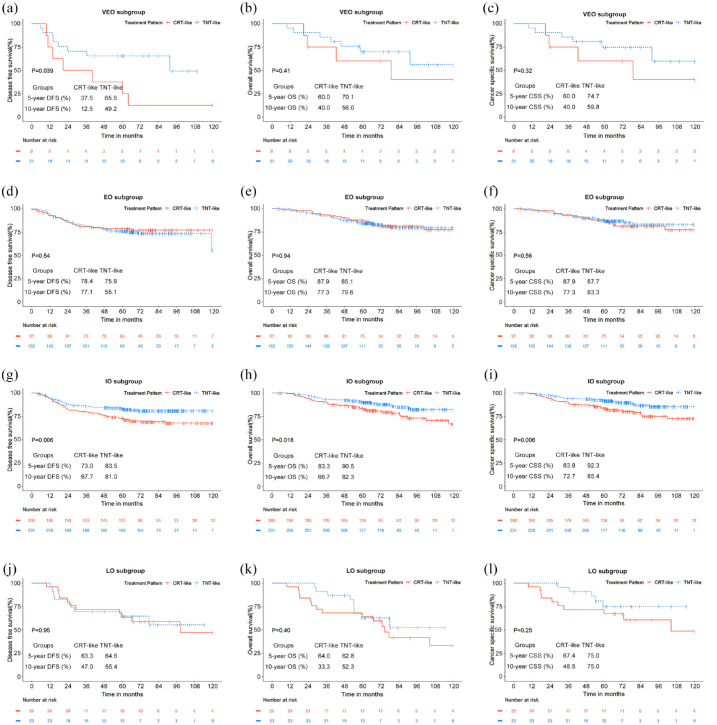
Results: There were more female VEO patients than males, more mucinous adenocarcinoma, signet-ring cell carcinoma, pre-treatment cT4 stage, and higher pre-treatment serum carbohydrate antigen 19-9 compared with the other three groups. VEO patients had the worst survival with the highest RC-related mortality (34.5%), recurrence (13.8%), and metastasis (51.7%). LO patients had the highest non-RC-related mortality rate (16.6%). The Cox regression model showed VEO was a negative independent prognostic factor for disease-free survival [DFS, hazard ratio (HR): 2.830, 95% confidence interval (CI): 1.633-4.904, p < 0.001], distant metastasis-free survival (DMFS, HR: 2.969, 95% CI: 1.720-5.127, p < 0.001), overall survival (OS, HR: 2.164, 95% CI: 1.102-4.249, p = 0.025), and cancer-specific survival (CSS, HR: 2.321, 95% CI: 1.145-4.705, p = 0.020). LO was a negative independent factor on DFS (HR: 1.800, 95% CI: 1.113-2.911, p = 0.017), DMFS (HR: 1.903, 95% CI: 1.150-3.149, p = 0.012), OS (HR: 2.856, 95% CI: 1.745-4.583, p < 0.001), and CSS (HR: 2.248, 95% CI: 1.282-3.942, p = 0.005). VEO patients had better survival in the total neoadjuvant therapy-like (TNT-like) pattern on DFS (p = 0.039). IO patients receiving TNT-like patterns had better survival on DFS, OS, and CSS (p = 0.006, p = 0.018, p = 0.006, respectively).
Conclusion: In stage III RC, VEO patients exhibited unique clinicopathological characteristics, with VEO a negative independent prognostic factor for DFS, DMFS, OS, and CSS. VEO and IO patients may benefit from a TNT-like treatment pattern.
Keywords: onset age; prognosis; rectal cancer; stage III; total neoadjuvant therapy.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin 2017; 67: 177–193. - PubMed
-
- Arshad HMS, Kabir C, Tetangco E, et al. Racial disparities in clinical presentation and survival times among young-onset colorectal adenocarcinoma. Dig Dis Sci 2017; 62: 2526–2531. - PubMed
-
- Lui RN, Tsoi KKF, Ho JMW, et al. Global increasing incidence of young-onset colorectal cancer across 5 continents: a joinpoint regression analysis of 1,922,167 cases. Cancer Epidemiol Biomarkers Prev 2019; 28: 1275–1282. - PubMed
LinkOut - more resources
Full Text Sources
