

Surgical Outcome in Bilateral Inguinal Hernia Repair: Laparoscopic Total Extraperitoneal Approach (TEP) as Best Approach?
- PMID: 38348087
- PMCID: PMC10859215
- DOI: 10.26574/maedica.2023.18.4.598
Surgical Outcome in Bilateral Inguinal Hernia Repair: Laparoscopic Total Extraperitoneal Approach (TEP) as Best Approach?
Abstract
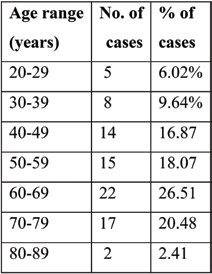
Introduction: Bilateral inguinal hernia is a distinct entity in the inguinal hernia category. Open and minimally invasive techniques for the treatment of bilateral inguinal hernia have been previously described. If resources and surgeon expertise are available, guidelines recommend laparoscopic repair for this entity. Methods:We analyzed data from 83 patients who underwent laparoscopic inguinal hernia repair (total extraperitoneal repair - TEP) of 158 hernias (146 inguinal hernias and 12 other types). Patients had bilateral symptomatic hernias. Results:Male predominance, with a mean age of 56.7 years, was noted. Lateral hernias (according to EHS classification) were prevalent (71.08%). In the majority of cases (77.11%), meshes made up of a custom polypropylene monofilament mesh were used, followed by Bard 3D Max mesh and Ultralight mesh. Regarding postoperative complications, seroma was the most frequently encountered one in our series (7.23%), followed by urinary retention and 'feeling' of mesh (2.41%). Hydrocele, wound hematoma, cord hematoma and chronic pain were seen in 1.20% of patients. No wound infections were observed. The average operative time was 97.77 minutes (SD=17.08); when associated surgery was present, it prolonged the operative time, and we found statistical significance (p=0.002). Similarly, the presence of recurrent hernia extended the operative time, which was found to be statistically significant (p=0.003). The conversion rate in our data was 2.41%. Drainage, which was performed in 13 patients (15.66%), decreased the incidence of complications, especially seroma (p=0.026). The mean length of hospital stay was 2.93 days (SD=1.81), with most of the patients having been discharged on the second postoperative day (37.35%). Only one recurrence was identified (1.20%). Conclusion:The laparoscopic approach for bilateral inguinal hernia treatment is feasible and has been proven to be advantageous. Our study emphasizes that the TEP procedure has low rates of complications, conversion and recurrence; hence, we recommend bilateral hernia repair.
Figures














References
-
- Poelman MM, van den Heuvel B, Deelder JD, et al. EAES Consensus Development Conference on endoscopic repair of groin hernias. Surg Endosc. 2013;27:3505–3519. - PubMed
-
- Hiratsuka T, Shigemitsu Y, Etoh T, et al. Appropriate mesh size in the totally extraperitoneal repair of groin hernias based on the intraoperative measurement of the myopectineal orifice. Surg Endosc. 2021;35:2126–2133. - PubMed
-
- Miserez M, Alexandre JH, Campanelli G, et al. The European hernia society groin hernia classification: simple and easy to remember. Hernia. 2007;11:113–116. - PubMed
Publication types
LinkOut - more resources
Full Text Sources