

Association of EEG Background With Diffusion-Weighted Magnetic Resonance Neuroimaging and Short-Term Outcomes After Pediatric Cardiac Arrest
- PMID: 38350044
- PMCID: PMC11384654
- DOI: 10.1212/WNL.0000000000209134
Association of EEG Background With Diffusion-Weighted Magnetic Resonance Neuroimaging and Short-Term Outcomes After Pediatric Cardiac Arrest
Abstract
Background and objectives: EEG and MRI features are independently associated with pediatric cardiac arrest (CA) outcomes, but it is unclear whether their combination improves outcome prediction. We aimed to assess the association of early EEG background category with MRI ischemia after pediatric CA and determine whether addition of MRI ischemia to EEG background features and clinical variables improves short-term outcome prediction.
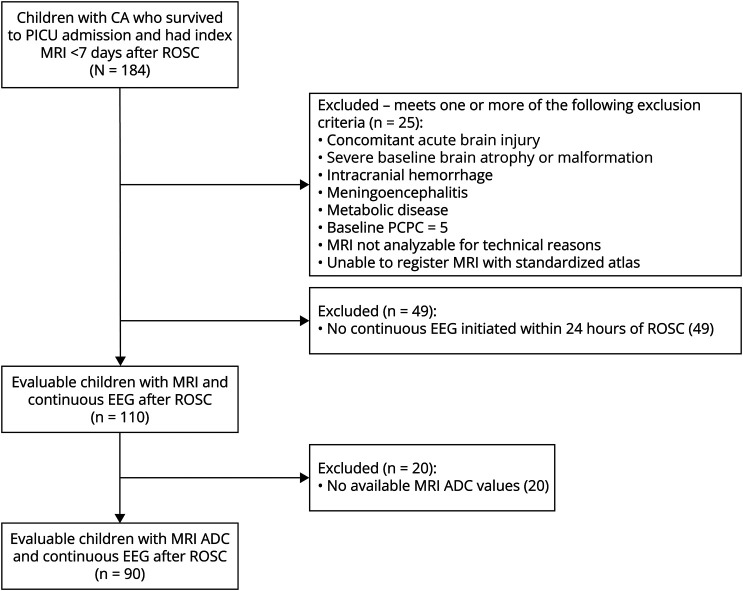
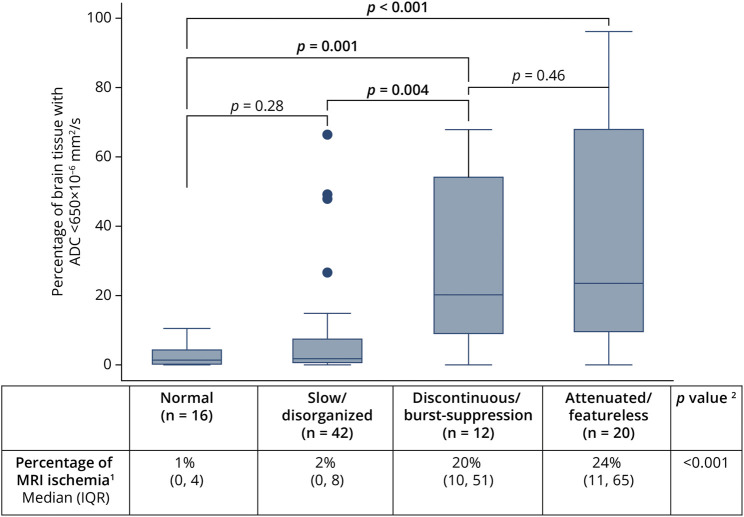
Methods: This was a single-center retrospective cohort study of pediatric CA with EEG initiated ≤24 hours and MRI obtained ≤7 days of return of spontaneous circulation. Initial EEG background was categorized as normal, slow/disorganized, discontinuous/burst-suppression, or attenuated-featureless. MRI ischemia was defined as percentage of brain tissue with apparent diffusion coefficient (ADC) <650 × 10-6 mm2/s and categorized as high (≥10%) or low (<10%). Outcomes were mortality and unfavorable neurologic outcome (Pediatric Cerebral Performance Category increase ≥1 from baseline resulting in ICU discharge score ≥3). The Kruskal-Wallis test evaluated the association of EEG with MRI. Area under the receiver operating characteristic (AUROC) curve evaluated predictive accuracy. Logistic regression and likelihood ratio tests assessed multivariable outcome prediction.
Results: We evaluated 90 individuals. EEG background was normal in 16 (18%), slow/disorganized in 42 (47%), discontinuous/burst-suppressed in 12 (13%), and attenuated-featureless in 20 (22%) individuals. The median percentage of MRI ischemia was 5% (interquartile range 1-18); 32 (36%) individuals had high MRI ischemia burden. Twenty-eight (31%) individuals died, and 58 (64%) had unfavorable neurologic outcome. Worse EEG background category was associated with more MRI ischemia (p < 0.001). The combination of EEG background and MRI ischemia burden had higher predictive accuracy than EEG alone (AUROC: mortality: 0.92 vs 0.87, p = 0.03) or MRI alone (AUROC: mortality: 0.92 vs 0.84, p = 0.02; unfavorable: 0.83 vs 0.73, p < 0.01). Addition of percentage of MRI ischemia to clinical variables and EEG background category improved prediction for mortality (χ2 = 19.1, p < 0.001) and unfavorable neurologic outcome (χ2 = 4.8, p = 0.03) and achieved high predictive accuracy (AUROC: mortality: 0.97; unfavorable: 0.92).
Discussion: Early EEG background category was associated with MRI ischemia after pediatric CA. Combining EEG and MRI data yielded higher outcome predictive accuracy than either modality alone. The addition of MRI ischemia to clinical variables and EEG background improved short-term outcome prediction.
Conflict of interest statement
A.M. Bach reports no disclosures relevant to the manuscript. The institution of M.P. Kirschen has received research support from NIH. F.W. Fung reports no disclosures relevant to the manuscript. N.S. Abend has received personal compensation in the range of $5,000–$9,999 for serving as a consultant for Epilepsy Foundation, the institution of N.S. Abend has received research support from NIH, the institution of N.S. Abend has received research support from PCORI, and N.S. Abend has received publishing royalties from a publication relating to health care. S. Ampah reports no disclosures relevant to the manuscript. A. Mondal reports no disclosures relevant to the manuscript. J. Huh reports no disclosures relevant to the manuscript. S.-S.L. Chen reports no disclosures relevant to the manuscript. The institution of Dr. Yuan has received research support from Masimo Corp. K. Graham reports no disclosures relevant to the manuscript. J.I. Berman has received personal compensation in the range of $10,000–$49,999 for serving as a Consultant for McGowan Associates. J.I. Berman has received personal compensation in the range of $10,000–$49,999 for serving as an Expert Witness for McGowan Associates. A. Vossough has received personal compensation in the range of $500–$4,999 for serving as a Consultant for Syneos Health, has received personal compensation in the range of $0–$499 for serving on a Scientific Advisory or Data Safety Monitoring board for DeepSight, and has received publishing royalties from a publication relating to health care. A.A. Topjian has received personal compensation in the range of $5,000–$9,999 for serving as an Expert Witness for plantiff and defense. Go to
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical