

Intensive training programme for ultrasound-guided minimally invasive synovial tissue biopsy on knees and wrists in different phases of inflammation
- PMID: 38351051
- PMCID: PMC10868172
- DOI: 10.1136/rmdopen-2023-003705
Intensive training programme for ultrasound-guided minimally invasive synovial tissue biopsy on knees and wrists in different phases of inflammation
Abstract
Objectives: To develop an intensive training programme for ultrasound (US)-guided synovial tissue (ST) biopsy on knees and wrists in inflammatory arthritis and to assess the learning curve, patient tolerability, sample quality and trainees' expectations.
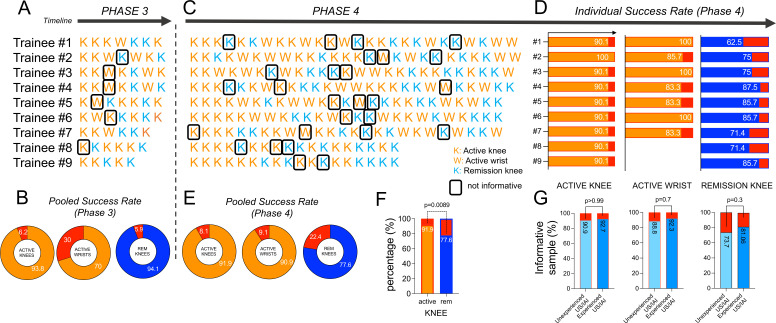
Methods: Active or remission rheumatoid arthritis patients were enrolled. Nine trainees joined the 4-month programme in a centre experienced in performing US-guided ST biopsies consisting of four sequential phases: (1) observation, (2) performance of guided step-by-step phases, (3) execution of the whole procedure on paired joints (knees or wrists) of the same patient in parallel with the trainer and (4) performance of the procedure autonomously. Sample representativity was assessed by histology, and procedure-related adverse events were recorded. Before and after the programme, trainees' expectations and perceptions were collected.
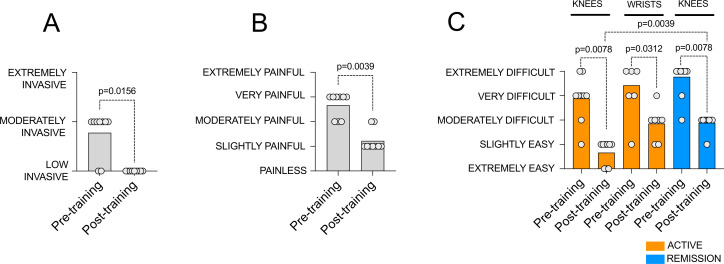
Results: 328 ST biopsy procedures were included. The rate of trainees' informative samples was: (1) comparable to the trainers in active and remission knees, but lower in active wrists (70% for trainees vs 100% for trainers, p=0.06) in phase 3; (2) excellent on active knees and wrists (91.9% and 90.9% respectively) but lower (77.6%, p=0.0089) on remission knees in phase 4. Procedures performed by trainees did not affect patient tolerability. Trainees' expectations about procedure-related invasiveness and pain infliction decreased while the difficulty of procedure execution on active wrists and remission knees remained perceived as moderately difficult.
Conclusions: This intensive training programme develops advanced skills in the performance of US-guided ST biopsy on knees and wrists, yielding high-quality specimens available for basic and translational studies on inflammatory joint diseases.
Keywords: Arthritis, Rheumatoid; Synovitis; Ultrasonography.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
-
- Humby F, Durez P, Buch MH, et al. . Rituximab versus tocilizumab in anti-TNF inadequate responder patients with rheumatoid arthritis (R4RA): 16-week outcomes of a stratified, biopsy-driven, multicentre, open-label, phase 4 randomised controlled trial. The Lancet 2021;397:305–17. 10.1016/S0140-6736(20)32341-2 - DOI - PMC - PubMed
-
- Alivernini S, Tolusso B, Petricca L, et al. . Synovial features of patients with rheumatoid arthritis and psoriatic arthritis in clinical and ultrasound remission differ under anti-TNF therapy: a clue to interpret different chances of relapse after clinical remission? Ann Rheum Dis 2017;76:1228–36. 10.1136/annrheumdis-2016-210424 - DOI - PMC - PubMed
-
- Alivernini S, Peluso G, Fedele AL, et al. . Tapering and discontinuation of TNF-α blockers without disease relapse using ultrasonography as a tool to identify patients with rheumatoid arthritis in clinical and histological remission. Arthritis Res Ther 2016;18:39. 10.1186/s13075-016-0927-z - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources