

Trajectories of resting energy expenditure and performance of predictive equations in children hospitalized with an acute illness and malnutrition: a longitudinal study
- PMID: 38351162
- PMCID: PMC10864294
- DOI: 10.1038/s41598-024-53791-w
Trajectories of resting energy expenditure and performance of predictive equations in children hospitalized with an acute illness and malnutrition: a longitudinal study
Abstract
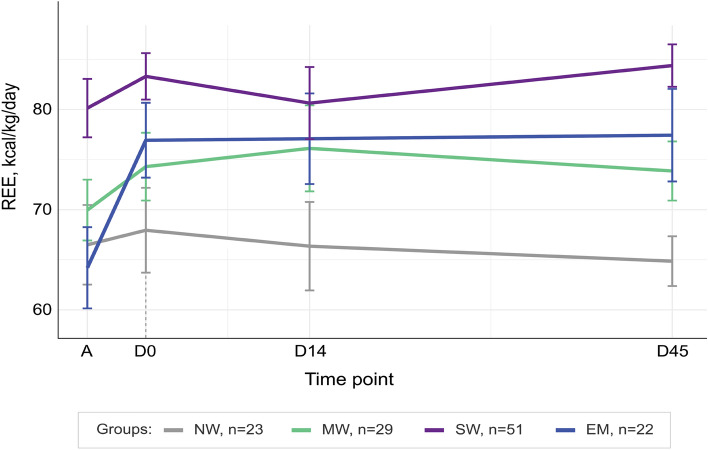
There is scarce data on energy expenditure in ill children with different degrees of malnutrition. This study aimed to determine resting energy expenditure (REE) trajectories in hospitalized malnourished children during and after hospitalization. We followed a cohort of children in Bangladesh and Malawi (2-23 months) with: no wasting (NW); moderate wasting (MW), severe wasting (SW), or edematous malnutrition (EM). REE was measured by indirect calorimetry at admission, discharge, 14-and-45-days post-discharge. 125 children (NW, n = 23; MW, n = 29; SW, n = 51; EM, n = 22), median age 9 (IQR 6, 14) months, provided 401 REE measurements. At admission, the REE of children with NW and MW was 67 (95% CI [58, 75]) and 70 (95% CI [63, 76]) kcal/kg/day, respectively, while REE in children with SW was higher, 79 kcal/kg/day (95% CI [74, 84], p = 0.018), than NW. REE in these groups was stable over time. In children with EM, REE increased from admission to discharge (65 kcal/kg/day, 95% CI [56, 73]) to 79 (95% CI [72, 86], p = 0.0014) and was stable hereafter. Predictive equations underestimated REE in 92% of participants at all time points. Recommended feeding targets during the acute phase of illness in severely malnourished children exceeded REE. Acutely ill malnourished children are at risk of being overfed when implementing current international guidelines.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Hossain M, et al. Efficacy of world health organization guideline in facility-based reduction of mortality in severely malnourished children from low and middle income countries: A systematic review and meta-analysis. J. Paediatr. Child Health. 2017;53:474–479. doi: 10.1111/jpc.13443. - DOI - PubMed
-
- Veldscholte K, Joosten K, Jotterand Chaparro C. Energy expenditure in critically ill children. Pediatr. Crit. Care Med. 2020;8:264–267. - PubMed
-
- WHO . Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children. World Health Organization; 2013. - PubMed
-
- WHO . Management of Severe Malnutrition: A Manual for Physicians and other Senior Health Workers. World Health Organization; 1999.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
