

Tourniquet on the low segment of the uterus reduces blood loss in postpartum hemorrhage during hysterectomy for placenta accreta: Old but gold
- PMID: 38351966
- PMCID: PMC10862398
- DOI: 10.1016/j.eurox.2024.100285
Tourniquet on the low segment of the uterus reduces blood loss in postpartum hemorrhage during hysterectomy for placenta accreta: Old but gold
Abstract
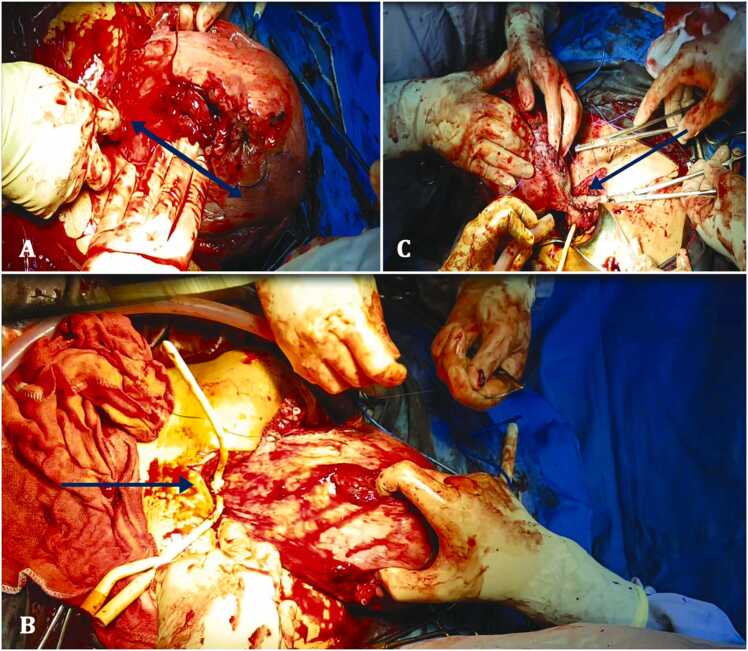
Objectives: To investigate the feasibility, safety, and efficiency after application of a cervical tourniquet during caesarian hysterectomy owing to placenta accreta.
Study design: It was a monocentric prospective observational study for 3 years. Patients were allocated into two group: Group Tourniquet: (TG) in which a cervical tourniquet was systematically applied during hysterectomy, control group (CG) when the caesarian hysterectomy was performed without.
Results: 20 patients in the TG and 23 patients in the CG. Tourniquet application significantly reduced per operative estimated blood loss volume (TG: 530 ± 135 vs 940 ± 120 ml in the CG, p = 0.0074), ΔHB (0.6 [0.3-1.9] vs 2.5[2.5-3.6] g/dl in the CG, p = 0.006) RBC transfusion requirements' (TG: 2 ± 1.7 vs 4.3 ± 2.1 units in the CG, p = 0.046) procedure duration (TG: 98 ± 21 vs 137 ± 33 min in the CG, p = 0.015), clotting disorders (TG: 1 (5%) vs 6 (26,1%) in the CG, p = 0.013) and the incidence of bladder wounds (TG: 1 (5%) vs 5 (21,7%) in the CG, p = 0.048). There was no significant difference regarding ICU transfer rate (TG: 16 (80%) vs 20 (86.9%) in the CG, p = 0.53) or length of stay (TG: 1.4 [2,3] vs 2.3 [1-4] days in the CG, p = 0.615) and digestive wound (TG: 0 vs 2 (8,7%) in the CG, p = 0.641).
Conclusion: In case of a radical management of placenta accreta. A strategy that involves the application of a cervical Tourniquet should be considered as a feasible, safe and above all efficient alternative to prevent blood spoliation.
Keywords: Blood loss; Hemoglobin variation; Maternal morbidity; Placenta accreta; Postpartum hemorrhage; Tourniquet.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Solheim K.N., Esakoff T.F., Little S.E., Cheng Y.W., Sparks T.N., Caughey A.B. The effect of cesarean delivery rates on the future incidence of placenta previa, placenta accreta, and maternal mortality. J Matern-Fetal Neonatal Med J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. 2011;24(11):1341–1346. - PubMed
-
- Bretelle F., Courbière B., Mazouni C., et al. Management of placenta accreta: morbidity and outcome. Eur J Obstet Gynecol Reprod Biol. 2007;133(1):34–39. - PubMed
-
- Hull A.D., Moore T.R. Multiple repeat cesareans and the threat of placenta accreta: incidence, diagnosis, management. Clin Perinatol. 2011;38(2):285–296. - PubMed
-
- Jauniaux E., Burton G.J. Pathophysiology of placenta accreta spectrum disorders: a review of current findings. Clin Obstet Gynecol. 2018 - PubMed
-
- Einerson B.D., Branch D.W. Surgical management of placenta accreta spectrum. Clin Obstet Gynecol. 2018 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
