

Endoscopic port access resection of left atrial myxoma: Clinical outcomes and a single surgeon's learning curve experience
- PMID: 38352019
- PMCID: PMC10859656
- DOI: 10.1016/j.xjtc.2023.11.014
Endoscopic port access resection of left atrial myxoma: Clinical outcomes and a single surgeon's learning curve experience
Abstract
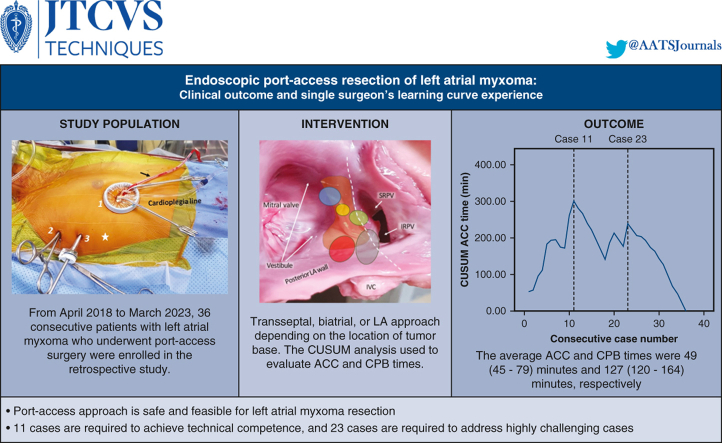
Objectives: To evaluate the safety and efficacy of the port access approach for left atrial (LA) myxoma resection and to analyze the learning curve for this procedure.
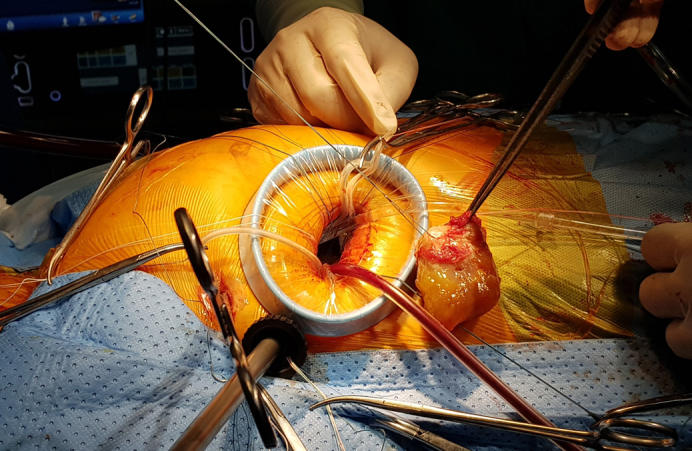
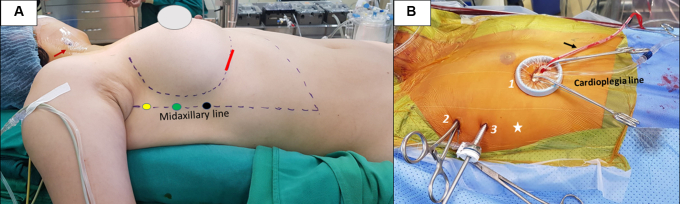
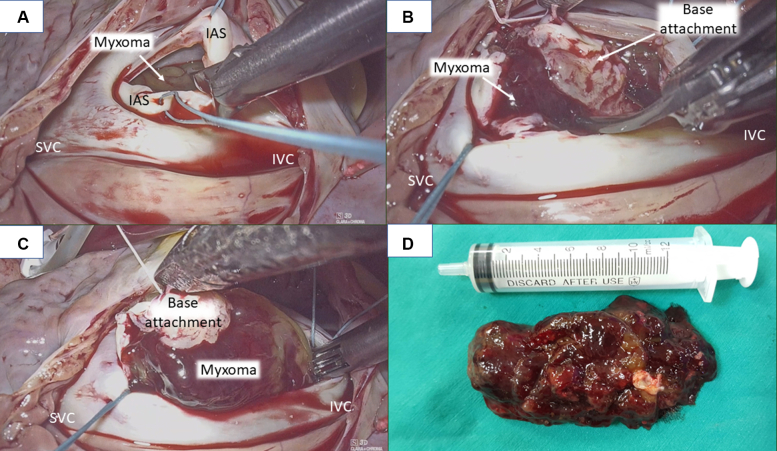
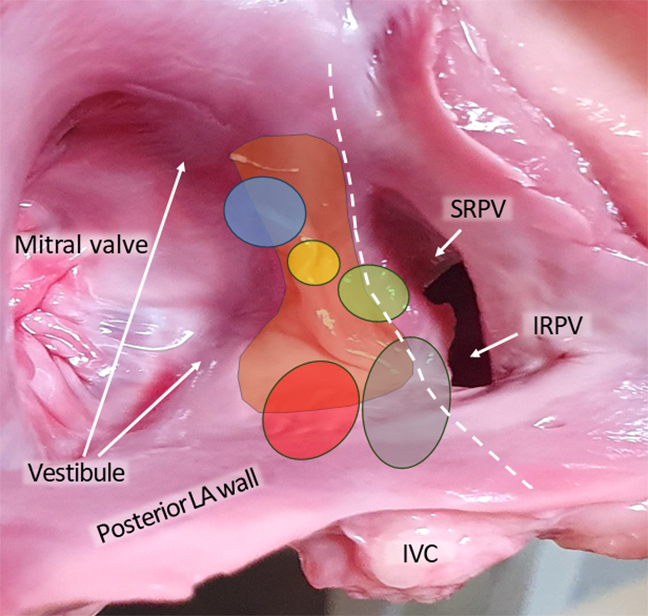
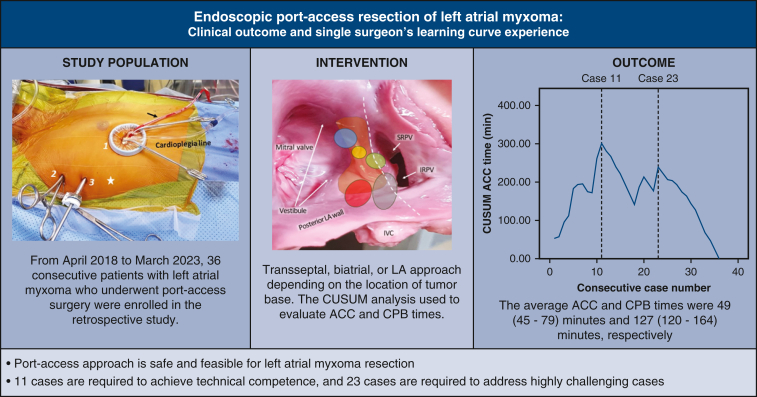
Methods: Thirty-six consecutive patients with LA myxoma who underwent port access surgery between April 2018 and March 2023 were enrolled in this retrospective study. The procedure included (1) unilateral or bilateral femoral artery cannulation; (2) the use of three 5-mm trocars and a 20- to 30-mm port; (3) a transseptal, biatrial, or LA approach depending on the location of the tumor base; and (4) complete or subendocardial tumor resection. CUSUM analysis was used to evaluate the aortic cross-clamp (ACC) time and cardiopulmonary bypass (CPB) time learning curves. Variables among the learning curve phases were compared.
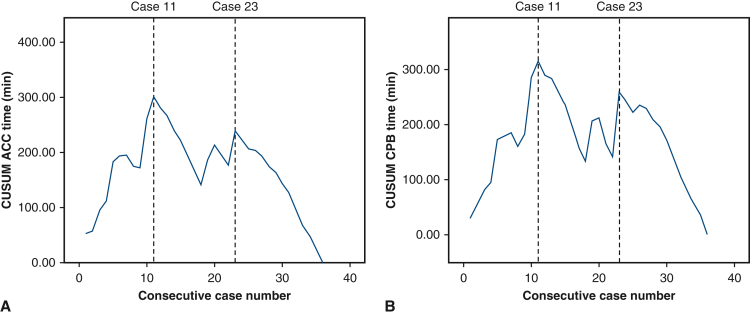
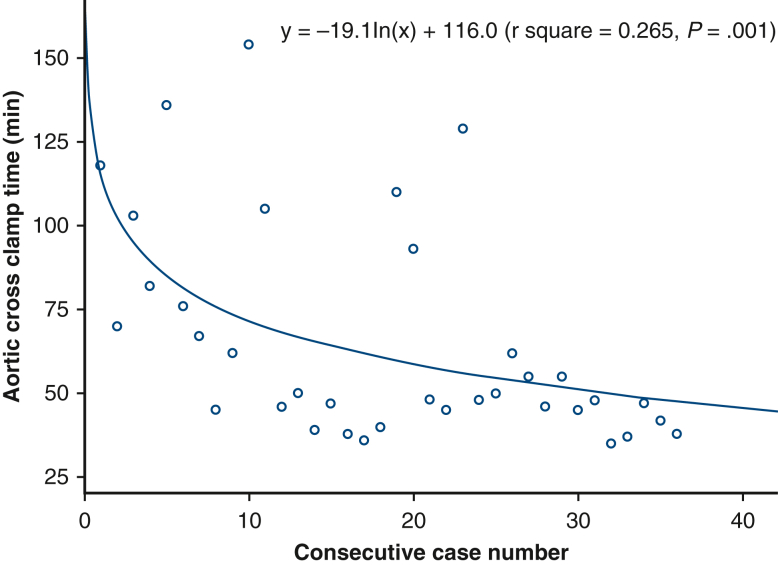
Results: The average ACC and CPB times were 49 (range, 45-79) minutes and 127 (range, 120-164) minutes, respectively. There was 1 case of conversion to sternotomy due to aortic root bleeding and 1 case of unilateral pulmonary edema. CUSUMACCtime analysis included 3 phases: phase I, the initial learning period (cases 1-11); phase II, the technical competence period (cases 12-23); and phase III, the challenging period (cases 24-36).
Conclusions: The port access approach is safe and feasible for LA myxoma resection. According to the learning curve analysis, 11 cases are required to achieve technical competence, and 23 cases are required to address highly challenging cases.
Keywords: learning curve; left atrial myxoma; minimally endoscopic cardiac surgery; port access.
© 2023 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures

Similar articles
-
Totally Endoscopic Atrial Septal Defect Repair on Beating Heart: Clinical Outcome and Single-Surgeon Learning Curve Experience.Innovations (Phila). 2023 Nov-Dec;18(6):574-582. doi: 10.1177/15569845231208457. Epub 2023 Nov 24. Innovations (Phila). 2023. PMID: 37997659
-
Routine endoscopic robotic cardiac tumor resection using an 8-mm working port and percutaneous cannulation.J Card Surg. 2022 Dec;37(12):4803-4807. doi: 10.1111/jocs.17166. Epub 2022 Nov 24. J Card Surg. 2022. PMID: 36423256
-
Minimally invasive video-assisted approach for left atrial myxoma resection.Interact Cardiovasc Thorac Surg. 2010 Jan;10(1):9-11. doi: 10.1510/icvts.2009.217232. Epub 2009 Oct 27. Interact Cardiovasc Thorac Surg. 2010. PMID: 19861325
-
Left atriotomy versus right atriotomy trans-septal approach for left atrial myxoma.J Int Med Res. 2010 Jan-Feb;38(1):276-81. doi: 10.1177/147323001003800132. J Int Med Res. 2010. PMID: 20233539
-
First Clinical Experience With Single-Port Robotic Transanal Minimally Invasive Surgery: Phase II Trial of the Initial 26 Cases.Dis Colon Rectum. 2021 Aug 1;64(8):1003-1013. doi: 10.1097/DCR.0000000000001999. Dis Colon Rectum. 2021. PMID: 34001709 Clinical Trial.
Cited by
-
Large left atrial myxoma with synchronous laryngeal squamous cell carcinoma: A case report.World J Cardiol. 2025 Feb 26;17(2):100952. doi: 10.4330/wjc.v17.i2.100952. World J Cardiol. 2025. PMID: 40061278 Free PMC article.
-
Robotic myxoma resection using an ultrasonic aspirator system.JTCVS Tech. 2024 Oct 16;29:100-102. doi: 10.1016/j.xjtc.2024.10.005. eCollection 2025 Feb. JTCVS Tech. 2024. PMID: 39991301 Free PMC article. No abstract available.
-
A Comprehensive Review of Cardiac Tumors: Imaging, Pathology, Treatment, and Challenges in the Third Millennium.Diagnostics (Basel). 2025 May 30;15(11):1390. doi: 10.3390/diagnostics15111390. Diagnostics (Basel). 2025. PMID: 40506961 Free PMC article. Review.
References
-
- Cohn L.H. 3rd ed. McGraw-Hill; 2007. Cardiac Surgery in the Adult.
-
- Grysman N.H., Watad A., Ofek E., Tzur B., Amital H. Rare myxoma arising from posterior wall of left atrium. Isr Med Assoc J. 2016;18:370–371. - PubMed
-
- Brant L.C., Mitu O., Gomide L., Bráulio R., Nunes M.C. Large atrial myxoma causing mitral obstruction and severe pulmonary hypertension. J Heart Valve Dis. 2011;20:357–359. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
